Wang Sheng-Fu, Huang Yu-Tung, Huang Chien-Hao, Chang Shang-Hung, Lin Chun-Yen
Division of Hepatology, Department of Gastroenterology and Hepatology, Chang-Gung Memorial Hospital, Linkou Medical Center, Taoyuan.
Center for Big Data Analytics and Statistics, Department of Medical Research and Development, Chang Gung Memorial Hospital, Linkou Medical Center, Taoyuan.
Ann Transl Med. 2020 Oct;8(19):1223. doi: 10.21037/atm-20-2444.
Various non-invasive markers predicting hepatic fibrosis are poor predictors of esophageal variceal bleeding (EVB). Elastography performs well but resource-limited. Controversy for small EV prevention also exists. We aim to investigate if a non-invasive marker could predict subsequent EVB within 1 and 2 years in patients with compensated liver cirrhosis (CLC), initial small EV without red-color sign (RCS), without use of non-selective beta-blockers (NSBB) and endoscopic variceal ligation (EVL). This marker would also be tested if it could help reduce use of NSBB, thereby avoiding potential side effects and saving medical costs.
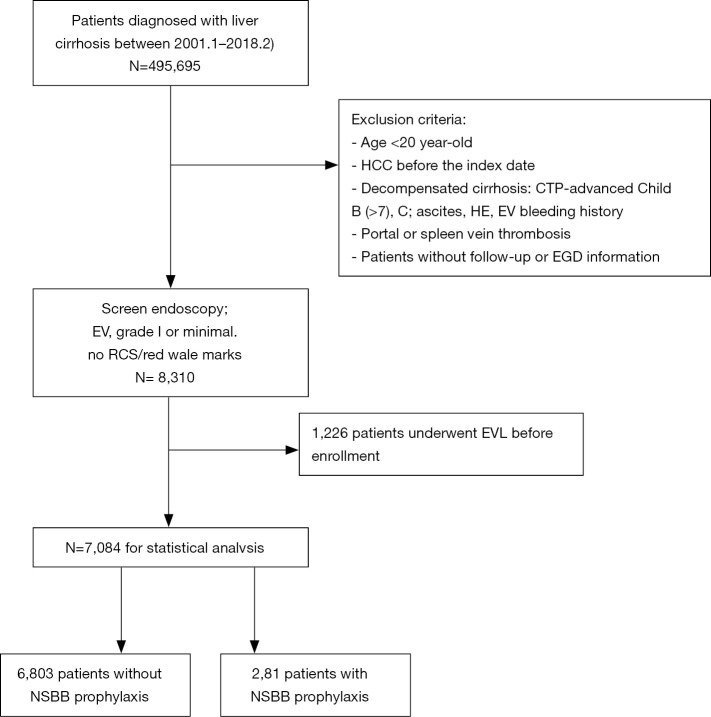
In this retrospective cohort study, 6,803 CLC patients fulfilling the inclusion-exclusion criteria were enrolled between 2001 and 2018, and were followed-up for 1 year, 2 years. The primary outcomes were subsequent EVB within 1 and 2 years of enrollment. Another 281 CLC patients with NSBB use were compared for additional outcome analysis.
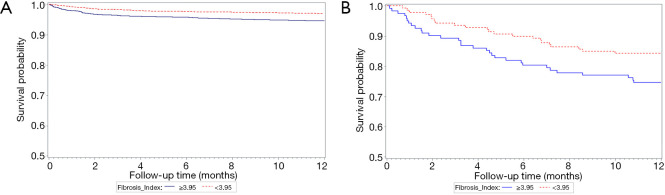
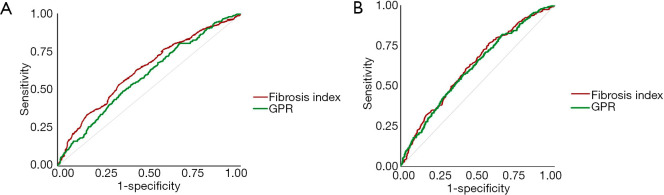
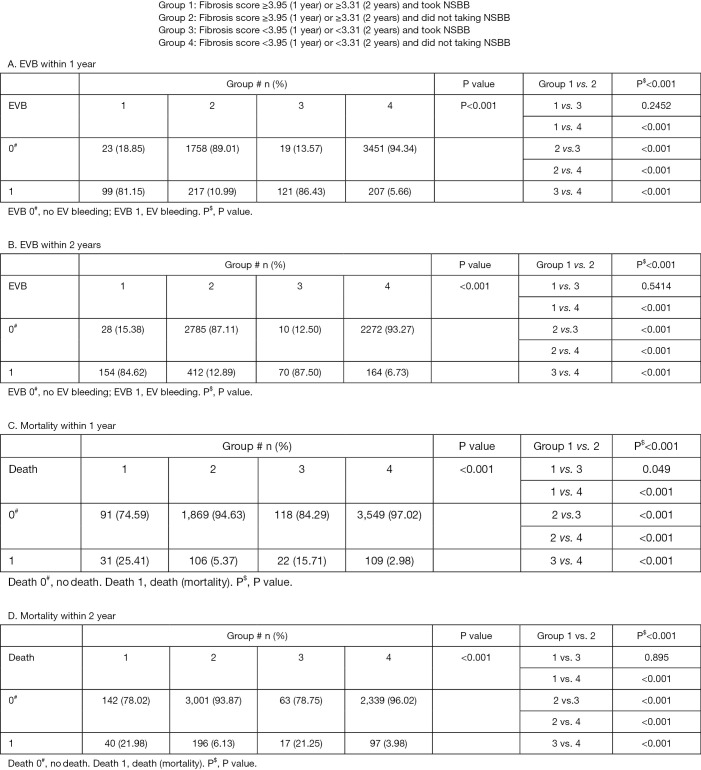
In total, 539 patients and 710 patients experienced EVB within 1 year and 2 years, respectively. The fibrosis index (FI) with cut-off value of 3.95 showed a negative predictive value (NPV) of 94.3% and an area under receiver operating characteristic (AUROC) of 62.95% for predicting subsequent EVB within 1 year. The EVB and mortality of patients with FI <3.95 and not taking NSBB were significantly lower than those of the other 3 groups. Similar results were demonstrated within 2 years.
In CLC patients with initial small EV and no RCS, low FI scores showed a high NPV and moderate AUROC in predicting subsequent EVB and mortalities, signifying clinically non-significant portal hypertension. Patients with low FI scores and not taking NSBB had significantly lowest EVB and mortality. The medical cost savings for cutting NSBB in these patients would be estimated at least $3 million per year in the U.S. Further randomized control trial study needed to validate this screening tool.
各种预测肝纤维化的非侵入性标志物对食管静脉曲张破裂出血(EVB)的预测效果不佳。弹性成像表现良好,但资源有限。对于预防小静脉曲张也存在争议。我们旨在研究一种非侵入性标志物能否在1年和2年内预测代偿期肝硬化(CLC)、初始小静脉曲张且无红色征(RCS)、未使用非选择性β受体阻滞剂(NSBB)和内镜下静脉曲张结扎术(EVL)的患者发生后续EVB。还将测试该标志物是否有助于减少NSBB的使用,从而避免潜在的副作用并节省医疗成本。
在这项回顾性队列研究中,2001年至2018年间纳入了6803例符合纳入排除标准的CLC患者,并进行了1年、2年的随访。主要结局是入组后1年和2年内发生的后续EVB。另外比较了281例使用NSBB的CLC患者以进行额外的结局分析。
总共分别有539例和710例患者在1年和2年内发生了EVB。纤维化指数(FI)截断值为3.95时,预测1年内后续EVB的阴性预测值(NPV)为94.3%,受试者工作特征曲线下面积(AUROC)为62.95%。FI<3.95且未服用NSBB的患者的EVB和死亡率显著低于其他3组。2年内也得到了类似结果。
在初始小静脉曲张且无RCS的CLC患者中,低FI评分在预测后续EVB和死亡率方面显示出高NPV和中等AUROC,表明临床上门静脉高压不显著。FI评分低且未服用NSBB的患者的EVB和死亡率显著最低。在美国,这些患者减少NSBB使用每年节省的医疗成本估计至少为300万美元。需要进一步的随机对照试验研究来验证这种筛查工具。