Heise Christian, Abou Ali Einas, Hasenclever Dirk, Auriemma Francesco, Gulla Aiste, Regner Sara, Gaujoux Sébastien, Hollenbach Marcus
Department of Medicine I-Gastroenterology, Pulmonology, Martin-Luther University Halle-Wittenberg, 06097 Halle, Germany.
Department of Gastroenterology, Digestive Oncology and Endoscopy, Cochin Hospital, Paris Descartes University, 75014 Paris, France.
J Clin Med. 2020 Nov 10;9(11):3622. doi: 10.3390/jcm9113622.
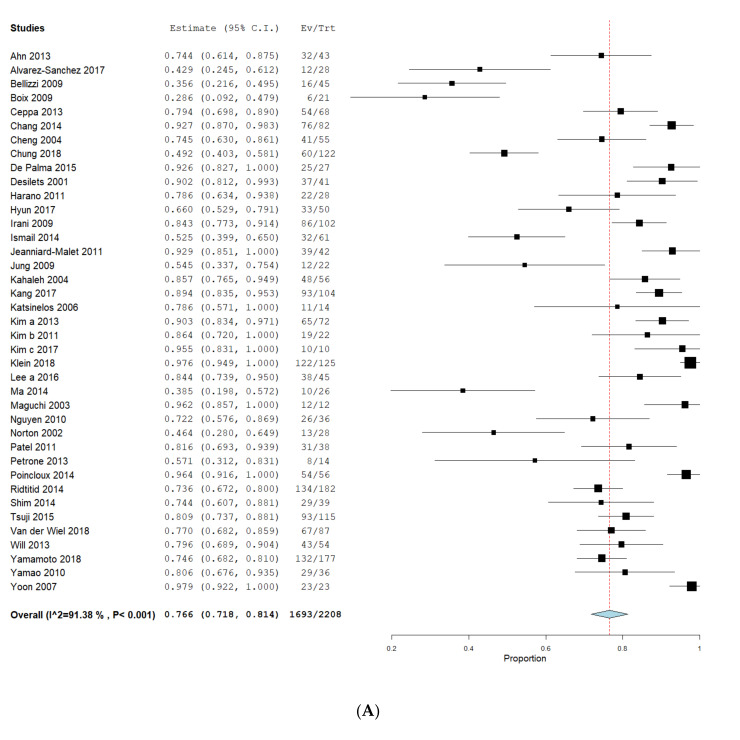
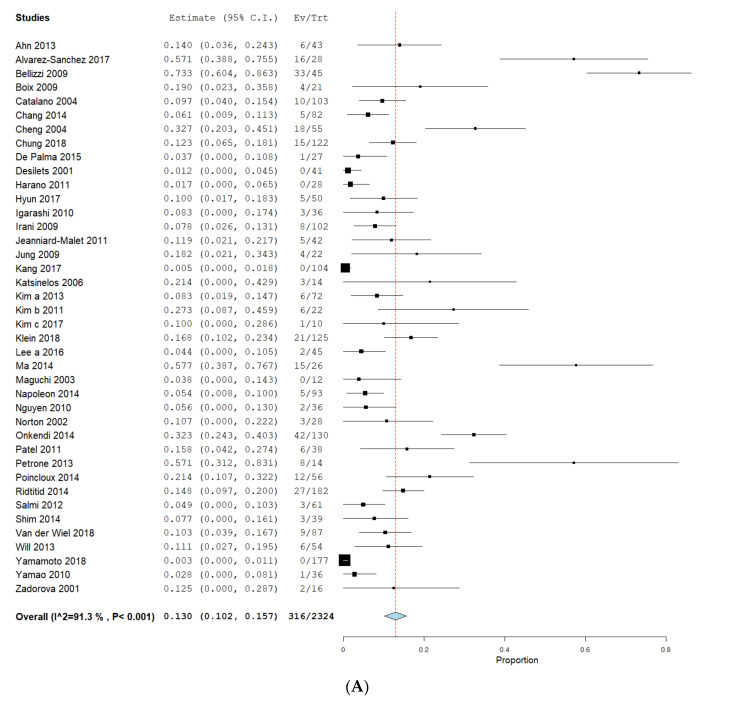
Ampullary lesions (ALs) can be treated by endoscopic (EA) or surgical ampullectomy (SA) or pancreaticoduodenectomy (PD). However, EA carries significant risk of incomplete resection while surgical interventions can lead to substantial morbidity. We performed a systematic review and meta-analysis for R0, adverse-events (AEs) and recurrence between EA, SA and PD. Electronic databases were searched from 1990 to 2018. Outcomes were calculated as pooled means using fixed and random-effects models and the Freeman-Tukey-Double-Arcsine-Proportion-model. We identified 59 independent studies. The pooled R0 rate was 76.6% (71.8-81.4%, I = 91.38%) for EA, 96.4% (93.6-99.2%, I = 37.8%) for SA and 98.9% (98.0-99.7%, I = 0%) for PD. AEs were 24.7% (19.8-29.6%, I = 86.4%), 28.3% (19.0-37.7%, I = 76.8%) and 44.7% (37.9-51.4%, I = 0%), respectively. Recurrences were registered in 13.0% (10.2-15.6%, I = 91.3%), 9.4% (4.8-14%, I = 57.3%) and 14.2% (9.5-18.9%, I = 0%). Differences between proportions were significant in R0 for EA compared to SA ( = 0.007) and PD ( = 0.022). AEs were statistically different only between EA and PD ( = 0.049) and recurrence showed no significance for EA/SA or EA/PD. Our data indicate an increased rate of complete resection in surgical interventions accompanied with a higher risk of complications. However, studies showed various sources of bias, limited quality of data and a significant heterogeneity, particularly in EA studies.
壶腹病变(ALs)可通过内镜下壶腹切除术(EA)、手术性壶腹切除术(SA)或胰十二指肠切除术(PD)进行治疗。然而,EA存在切除不完全的重大风险,而手术干预可能导致严重的发病率。我们对EA、SA和PD之间的R0、不良事件(AE)和复发情况进行了系统评价和荟萃分析。检索了1990年至2018年的电子数据库。使用固定效应模型和随机效应模型以及Freeman-Tukey-Double-Arcsine-Proportion模型将结果计算为合并均值。我们确定了59项独立研究。EA的合并R0率为76.6%(71.8 - 81.4%,I² = 91.38%),SA为96.4%(93.6 - 99.2%,I² = 37.8%),PD为98.9%(98.0 - 99.7%,I² = 0%)。AE发生率分别为24.7%(19.8 - 29.6%,I² = 86.4%)、28.3%(19.0 - 37.7%,I² = 76.8%)和44.7%(37.9 - 51.4%,I² = 0%)。复发率分别为13.0%(10.2 - 15.6%,I² = 91.3%)、9.4%(4.8 - 14%,I² = 57.3%)和14.2%(9.5 - 18.9%,I² = 0%)。EA与SA相比,R0的比例差异显著(P = 0.007),与PD相比也显著(P = 0.022)。AE仅在EA和PD之间存在统计学差异(P = 0.049),复发在EA/SA或EA/PD之间无显著差异。我们的数据表明,手术干预中完全切除率增加,但并发症风险更高。然而,研究显示存在各种偏倚来源、数据质量有限且存在显著异质性,尤其是在EA研究中。