Department of Anaesthesiology and Pain Medicine, Bern University Hospital, University of Bern, Bern, Switzerland.
Department of Anaesthesiology, University of Auckland, Auckland, New Zealand.
Can J Anaesth. 2020 Dec;67(12):1858-1878. doi: 10.1007/s12630-020-01820-3. Epub 2020 Nov 15.
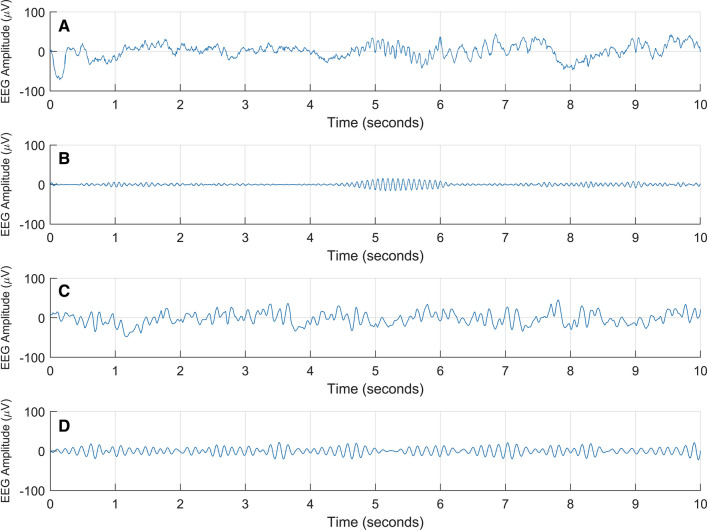
The electroencephalogram (EEG) provides a reliable reflection of the brain's electrical state, so it can reassure us that the anesthetic agents are actually reaching the patient's brain, and are having the desired effect. In most patients, the EEG changes somewhat predictably in response to propofol and volatile agents, so a frontal EEG channel can guide avoidance of insufficient and excessive administration of general anesthesia. Persistent alpha-spindles (around 10 Hz) phase-amplitude coupled with slow delta waves (around 1 Hz) are commonly seen during an "appropriate hypnotic state of general anesthesia". Such patterns can be appreciated from the EEG waveform or from the spectrogram (a colour-coded display of how the power in the various EEG frequencies changes with time). Nevertheless, there are exceptions to this. For example, administration of ketamine and nitrous oxide is generally not associated with the aforementioned alpha-spindle coupled with delta wave pattern. Also, some patients, including older adults and those with neurodegenerative disorders, are less predisposed to generate a strong electroencephalographic "alpha-spindle" pattern during general anesthesia. There might also be some rare instances when the frontal EEG shows a pattern suggestive of general anesthesia, while the patient has some awareness and is able to follow simple commands, albeit this is typically without obvious distress or memory formation. Thus, the frontal EEG alone, as currently analyzed, is an imperfect but clinically useful mirror, and more scientific insights will be needed before we can claim to have a reliable readout of brain "function" during general anesthesia.
脑电图(EEG)可靠地反映了大脑的电状态,因此可以使我们确信麻醉剂确实到达了患者的大脑,并产生了预期的效果。在大多数患者中,脑电图会对异丙酚和挥发性麻醉剂的反应发生可预测的变化,因此额部 EEG 通道可以指导避免全身麻醉剂的不足和过量给药。持续的阿尔法纺锤波(约 10 Hz)与缓慢的德尔塔波(约 1 Hz)相位幅度耦合,通常在“全身麻醉的适当催眠状态”中可见。这些模式可以从 EEG 波形或频谱图(以彩色显示 EEG 频率的功率随时间的变化)中得到。尽管如此,也有例外。例如,氯胺酮和一氧化二氮的给药通常与上述阿尔法纺锤波与德尔塔波模式无关。此外,一些患者,包括老年人和神经退行性疾病患者,在全身麻醉期间不太容易产生强烈的脑电图“阿尔法纺锤波”模式。也可能有一些罕见的情况,即额叶 EEG 显示出全身麻醉的模式,而患者有一定的意识并能够跟随简单的命令,尽管这通常没有明显的痛苦或记忆形成。因此,目前分析的额叶 EEG 只是一个不完美但临床有用的镜子,在我们能够声称对全身麻醉期间大脑“功能”有可靠的读数之前,还需要更多的科学洞察力。