Wu Wei, Deng Zhong, Alafate Wahafu, Wang Yichang, Xiang Jianyang, Zhu Lizhe, Li Bolin, Wang Maode, Wang Jia
Department of Neurosurgery, The First Affiliated Hospital of Xi'an Jiaotong University, Xi'an, China.
Center of Brain Science, The First Affiliated Hospital of Xi'an Jiaotong University, Xi'an, China.
Front Oncol. 2020 Oct 21;10:1750. doi: 10.3389/fonc.2020.01750. eCollection 2020.
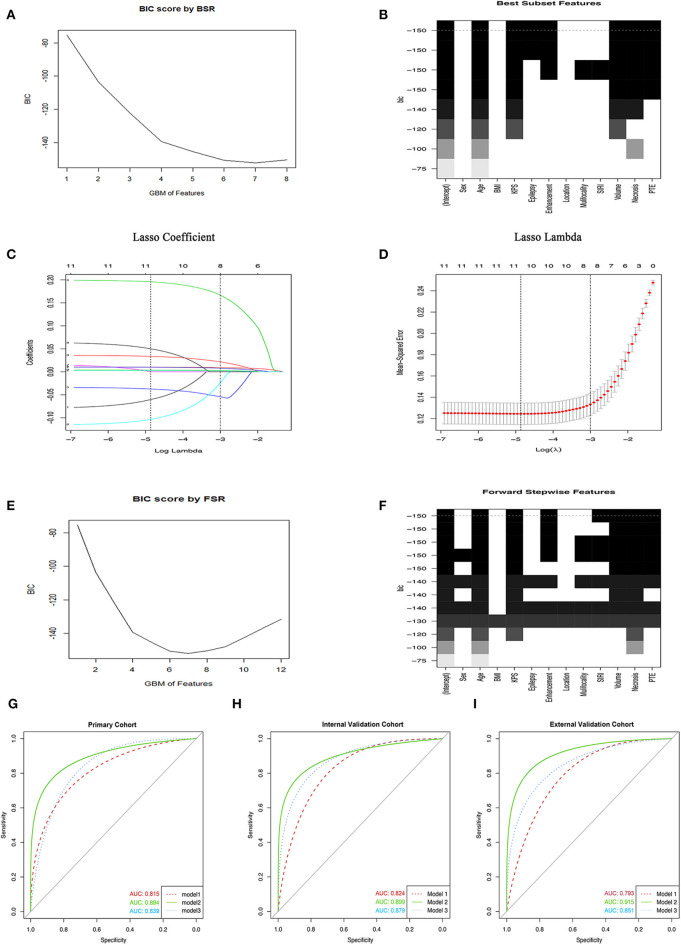
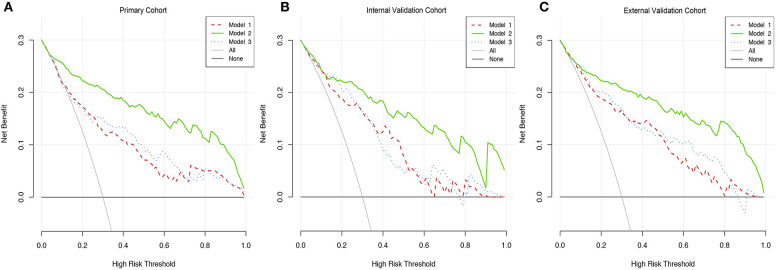
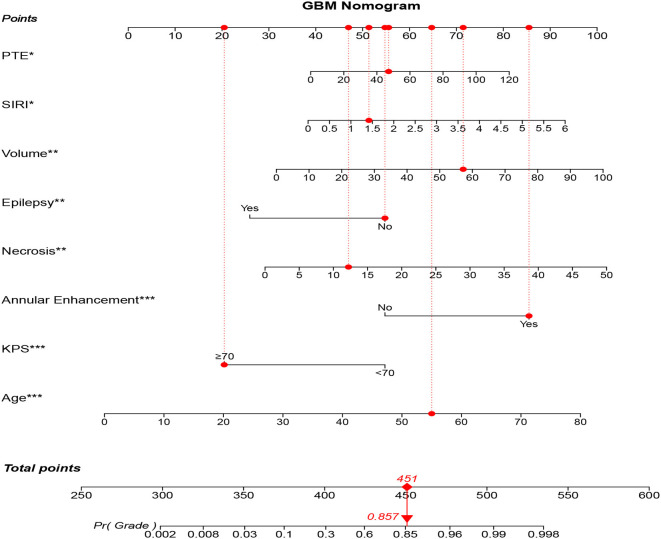
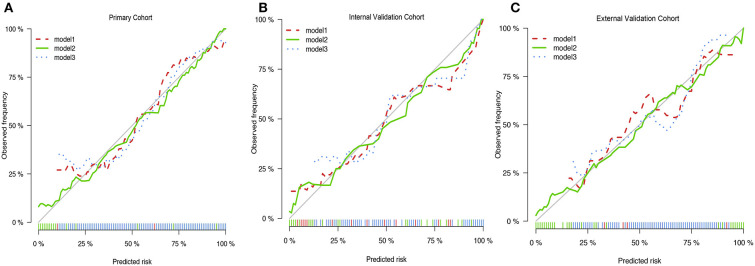
Traditional classification that divided gliomas into glioblastoma multiformes (GBM) and lower grade gliomas (LGG) based on pathological morphology has been challenged over the past decade by improvements in molecular stratification, however, the reproducibility and diagnostic accuracy of glioma classification still remains poor. This study aimed to establish and validate a novel nomogram for the preoperative diagnosis of GBM by using integrated data combined with feasible baseline characteristics and preoperative tests. The models were established in a primary cohort that included 259 glioma patients who had undergone surgical resection and were pathologically diagnosed from March 2014 to May 2016 in the First Affiliated Hospital of Xi'an Jiaotong University. The preoperative data were used to construct three models by the best subset regression, the forward stepwise regression, and the least absolute shrinkage and selection operator, and to furthermore establish the nomogram among those models. The assessment of nomogram was carried out by the discrimination and calibration in internal cohorts and external cohorts. Out of all three models, model 2 contained eight clinical-related variables, which exhibited the minimum Akaike Information Criterion (173.71) and maximum concordance index (0.894). Compared with the other two models, the integrated discrimination index for model 2 was significantly improved, indicating that the nomogram obtained from model 2 was the most appropriate model. Likewise, the nomogram showed great calibration and significant clinical benefit according to calibration curves and the decision curve analysis. In conclusion, our study showed a novel preoperative model that incorporated clinically relevant variables and imaging features with laboratory data that could be used for preoperative prediction in glioma patients, thus providing more reliable evidence for surgical decision-making.
基于病理形态学将胶质瘤分为多形性胶质母细胞瘤(GBM)和低级别胶质瘤(LGG)的传统分类方法,在过去十年中受到了分子分层技术进步的挑战,然而,胶质瘤分类的可重复性和诊断准确性仍然较差。本研究旨在通过整合可行的基线特征和术前检查数据,建立并验证一种用于GBM术前诊断的新型列线图。这些模型在一个主要队列中建立,该队列包括259例胶质瘤患者,他们于2014年3月至2016年5月在西安交通大学第一附属医院接受了手术切除并经病理诊断。术前数据通过最佳子集回归、向前逐步回归和最小绝对收缩与选择算子构建了三个模型,并在这些模型中进一步建立了列线图。通过内部队列和外部队列中的鉴别和校准对列线图进行评估。在所有三个模型中,模型2包含八个临床相关变量,其表现出最小的赤池信息准则(173.71)和最大的一致性指数(0.894)。与其他两个模型相比,模型2的综合鉴别指数显著提高,表明从模型2获得的列线图是最合适的模型。同样,根据校准曲线和决策曲线分析,列线图显示出良好的校准和显著的临床益处。总之,我们的研究展示了一种新型的术前模型,该模型将临床相关变量、影像特征与实验室数据相结合,可用于胶质瘤患者的术前预测,从而为手术决策提供更可靠的证据。