Clin Orthop Relat Res. 2021 May 1;479(5):1158-1166. doi: 10.1097/CORR.0000000000001568.
Delivering uninterrupted cancer treatment to patients with musculoskeletal tumors has been essential during the rapidly evolving coronavirus 2019 (COVID-19) pandemic, as delays in management can be detrimental. Currently, the risk of contracting COVID-19 in hospitals when admitted for surgery and the susceptibility due to adjuvant therapies and associated mortality due to COVID-19 is unknown, but knowledge of these potential risks would help treating clinicians provide appropriate cancer care.
QUESTIONS/PURPOSES: (1) What is the risk of hospital-acquired COVID-19 in patients with musculoskeletal tumors admitted for surgery during the initial period of the pandemic? (2) What is the associated mortality in patients with musculoskeletal tumors who have contracted COVID-19? (3) Are patients with musculoskeletal tumors who have had neoadjuvant therapy (chemotherapy or radiation) preoperatively at an increased risk of contracting COVID-19? (4) Is a higher American Society of Anesthesiologists (ASA) grade in patients with musculoskeletal tumors associated with an increased risk of contracting COVID-19 when admitted to the hospital for surgery?
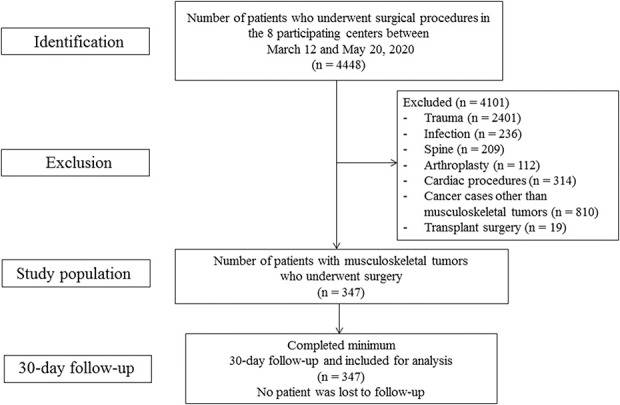
This retrospective, observational study analyzed patients with musculoskeletal tumors who underwent surgery in one of eight specialist centers in the United Kingdom, which included the five designated cancer centers in England, one specialist soft tissue sarcoma center, and two centers from Scotland between March 12, 2020 and May 20, 2020. A total of 347 patients were included, with a median (range) age of 53 years (10 to 94); 60% (207 of 347) were men, and the median ASA grade was II (I to IV). These patients had a median hospital stay of 8 days (0 to 53). Eighteen percent (61 of 347) of patients had received neoadjuvant therapy (8% [27] chemotherapy, 8% [28] radiation, 2% [6] chemotherapy and radiation) preoperatively. The decision to undergo surgery was made in adherence with United Kingdom National Health Service and national orthopaedic oncology guidelines, but specific data with regard to the number of patients within each category are not known. Fifty-nine percent (204 of 347) were negative in PCR testing done 48 hours before the surgical procedure; the remaining 41% (143 of 347) were treated before preoperative PCR testing was made mandatory, but these patients were asymptomatic. All patients were followed for 30 days postoperatively, and none were lost to follow-up during that period. The primary outcome of the study was contracting COVID-19 in the hospital after admission. The secondary outcome was associated mortality after contracting COVID-19 within 30 days of the surgical procedure. In addition, we assessed whether there is any association between ASA grade or neoadjuvant treatment and the chances of contracting COVID-19 in the hospital. Electronic patient record system and simple descriptive statistics were used to analyze both outcomes.
Four percent (12 of 347) of patients contracted COVID-19 in the hospital, and 1% (4 of 347) of patients died because of COVID-19-related complications. Patients with musculoskeletal tumors who contracted COVID-19 had increased mortality compared with patients who were asymptomatic or tested negative (odds ratio 55.33 [95% CI 10.60 to 289.01]; p < 0.001).With the numbers we had, we could not show that adjuvant therapy had any association with contracting COVID-19 while in the hospital (OR 0.94 [95% CI 0.20 to 4.38]; p = 0.93). Increased ASA grade was associated with an increased likelihood of contracting COVID-19 (OR 58 [95% CI 5 to 626]; p < 0.001).
Our results show that surgeons must be mindful and inform patients that those with musculoskeletal tumors are at risk of contracting COVID-19 while admitted to the hospital and some may succumb to it. Hospital administrators and governmental agencies should be aware that operations on patients with lower ASA grade appear to have lower risk and should consider restructuring service delivery to ensure that procedures are performed in designated COVID-19-restricted sites. These measures may reduce the likelihood of patients contracting the virus in the hospital, although we cannot confirm a benefit from this study. Future studies should seek to identify factors influencing these outcomes and also compare surgical complications in those patients with and without COVID-19.
Level III, therapeutic study.
在快速演变的 2019 年冠状病毒病(COVID-19)大流行期间,为患有肌肉骨骼肿瘤的患者提供不间断的癌症治疗至关重要,因为管理上的延迟可能会产生不利影响。目前,在因手术而住院期间,患者在医院感染 COVID-19 的风险以及因辅助治疗而感染的易感性和因 COVID-19 而导致的死亡率尚不清楚,但了解这些潜在风险将有助于治疗临床医生提供适当的癌症护理。
问题/目的:(1)在大流行初期,患有肌肉骨骼肿瘤并接受手术的患者在医院感染 COVID-19 的风险是多少?(2)患有肌肉骨骼肿瘤且已感染 COVID-19 的患者的相关死亡率是多少?(3)术前接受新辅助治疗(化疗或放疗)的患有肌肉骨骼肿瘤的患者是否更容易感染 COVID-19?(4)患有肌肉骨骼肿瘤的患者,其美国麻醉师协会(ASA)分级较高,在因手术而住院时是否更有可能感染 COVID-19?
本回顾性、观察性研究分析了在英国的 8 家专业中心之一接受手术的患有肌肉骨骼肿瘤的患者,其中包括英格兰的 5 家指定癌症中心、一家专门的软组织肉瘤中心和苏格兰的 2 家中心,时间为 2020 年 3 月 12 日至 2020 年 5 月 20 日。共纳入 347 例患者,中位(范围)年龄为 53 岁(10-94);60%(207/347)为男性,中位 ASA 分级为 II 级(I-IV 级)。这些患者的中位住院时间为 8 天(0-53)。18%(61/347)的患者术前接受了新辅助治疗(8%[27]化疗,8%[28]放疗,2%[6]化疗和放疗)。手术的决定是根据英国国家卫生服务和国家骨科肿瘤学指南做出的,但具体每个类别的患者数量不详。59%(204/347)的患者在手术前 48 小时进行的 PCR 检测中结果为阴性;其余 41%(143/347)在术前 PCR 检测成为强制性之前进行了治疗,但这些患者无症状。所有患者在术后 30 天内进行随访,在此期间无患者失访。研究的主要结局是患者在入院后在医院感染 COVID-19。次要结局是患者在手术后 30 天内因 COVID-19 相关并发症而死亡的相关死亡率。此外,我们还评估了 ASA 分级或新辅助治疗与患者在医院感染 COVID-19 的几率之间是否存在任何关联。使用电子患者记录系统和简单描述性统计对两个结局进行分析。
4%(12/347)的患者在医院感染 COVID-19,1%(4/347)的患者因 COVID-19 相关并发症而死亡。与无症状或检测结果为阴性的患者相比,患有肌肉骨骼肿瘤且感染 COVID-19 的患者死亡率更高(比值比 55.33[95%CI 10.60-289.01];p<0.001)。根据我们的数据,我们无法表明辅助治疗与患者在医院感染 COVID-19 之间存在任何关联(比值比 0.94[95%CI 0.20-4.38];p=0.93)。较高的 ASA 分级与感染 COVID-19 的几率增加相关(比值比 58[95%CI 5-626];p<0.001)。
我们的研究结果表明,外科医生必须注意并告知患有肌肉骨骼肿瘤的患者,他们在住院期间有感染 COVID-19 的风险,并且有些人可能会因此而死亡。医院管理人员和政府机构应意识到,ASA 分级较低的患者的手术风险似乎较低,应考虑调整服务交付,以确保在指定的 COVID-19 限制地点进行手术。这些措施可能会降低患者在医院感染病毒的可能性,尽管我们不能从这项研究中证实这种益处。未来的研究应寻求确定影响这些结果的因素,并比较患有和不患有 COVID-19 的患者的手术并发症。
III 级,治疗性研究。