Department of Chemical and Biomolecular Engineering, Institute for Medicine and Engineering, University of Pennsylvania, Philadelphia, Pennsylvania, United States of America.
Department of Trauma Surgery, University of Pennsylvania, Philadelphia, Pennsylvania, United States of America.
PLoS One. 2020 Nov 17;15(11):e0242166. doi: 10.1371/journal.pone.0242166. eCollection 2020.
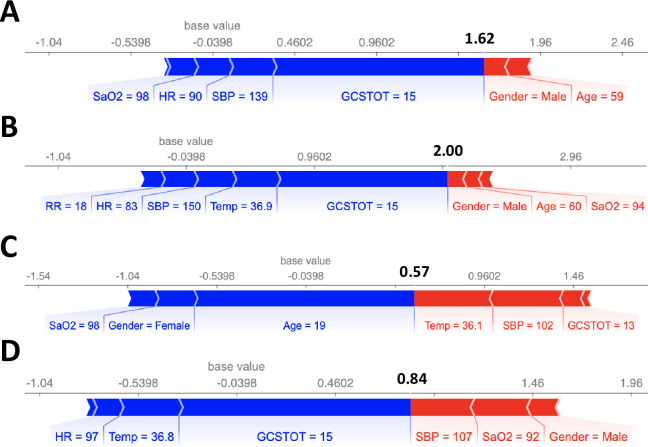
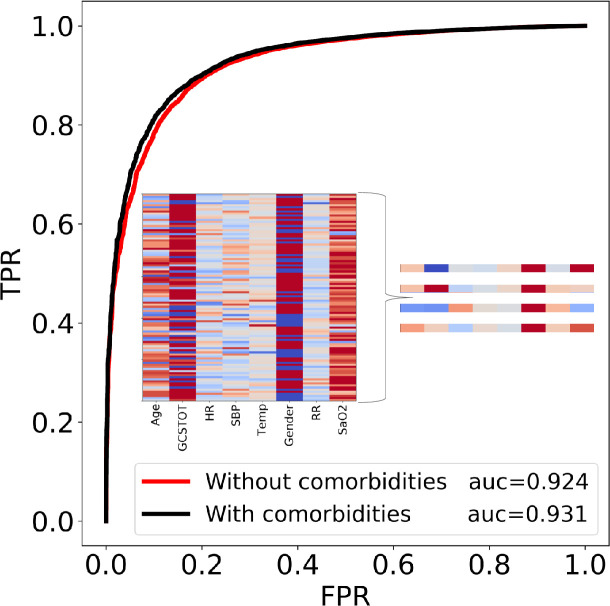
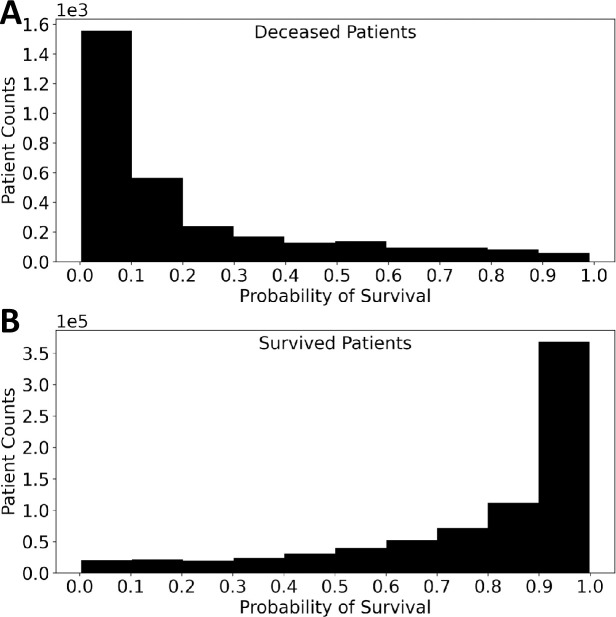
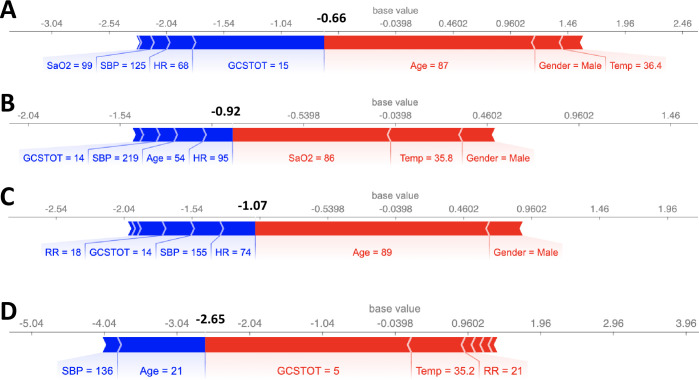
A 400-estimator gradient boosting classifier was trained to predict survival probabilities of trauma patients. The National Trauma Data Bank (NTDB) provided 799233 complete patient records (778303 survivors and 20930 deaths) each containing 32 features, a number further reduced to only 8 features via the permutation importance method. Importantly, the 8 features can all be readily determined at admission: systolic blood pressure, heart rate, respiratory rate, temperature, oxygen saturation, gender, age and Glasgow coma score. Since death was rare, a rebalanced training set was used to train the model. The model is able to predict a survival probability for any trauma patient and accurately distinguish between a deceased and survived patient in 92.4% of all cases. Partial dependence curves (Psurvival vs. feature value) obtained from the trained model revealed the global importance of Glasgow coma score, age, and systolic blood pressure while pulse rate, respiratory rate, temperature, oxygen saturation, and gender had more subtle single variable influences. Shapley values, which measure the relative contribution of each of the 8 features to individual patient risk, were computed for several patients and were able to quantify patient-specific warning signs. Using the NTDB to sample across numerous patient traumas and hospital protocols, the trained model and Shapley values rapidly provides quantitative insight into which combination of variables in an 8-dimensional space contributed most to each trauma patient's predicted global risk of death upon emergency room admission.
使用 400 个估计量的梯度提升分类器来预测创伤患者的生存概率。国家创伤数据库(NTDB)提供了 799233 份完整的患者记录(778303 名幸存者和 20930 名死亡者),每份记录包含 32 个特征,通过排列重要性方法进一步减少到只有 8 个特征。重要的是,这 8 个特征在入院时都可以很容易地确定:收缩压、心率、呼吸率、体温、血氧饱和度、性别、年龄和格拉斯哥昏迷评分。由于死亡人数较少,因此使用了再平衡的训练集来训练模型。该模型能够预测任何创伤患者的生存概率,并在 92.4%的情况下准确区分死亡和存活患者。从训练有素的模型中获得的部分依赖曲线(Psurvival 与特征值)显示了格拉斯哥昏迷评分、年龄和收缩压的全局重要性,而脉搏率、呼吸率、体温、血氧饱和度和性别则具有更细微的单变量影响。Shapley 值用于衡量 8 个特征中的每一个对个体患者风险的相对贡献,为几个患者计算了 Shapley 值,并能够量化患者特定的警告信号。通过使用 NTDB 在多个患者创伤和医院协议中进行抽样,训练有素的模型和 Shapley 值可以快速提供有关 8 维空间中哪些变量组合对每个创伤患者急诊入院时的全球死亡风险预测贡献最大的定量见解。