Department of Critical Care Medicine, The First Medical Centre, Chinese PLA General Hospital, Beijing 100853, People's Republic of China.
Institution of Hospital Management, Medical Innovation Research Division of Chinese PLA General Hospital, Beijing 100853, People's Republic of China.
Clin Interv Aging. 2020 Nov 9;15:2095-2107. doi: 10.2147/CIA.S273720. eCollection 2020.
Severe or critical patients with coronavirus disease 2019 (COVID-19) are at increased risk for developing acute kidney injury (AKI). However, the rate of AKI in patients of different severities and independent predictive factors associated with AKI are not well understood.
We enrolled 107 severely or critically ill elderly patients with COVID-19 who were admitted to the intensive care unit (ICU) in Wuhan, China. AKI was defined according to the 2012 KDIGO criteria. We explored the association between AKI and in-hospital mortality using logistic regression. A predictive nomogram was formulated to predict the AKI development of patients with COVID-19 based on multivariate logistic regression.
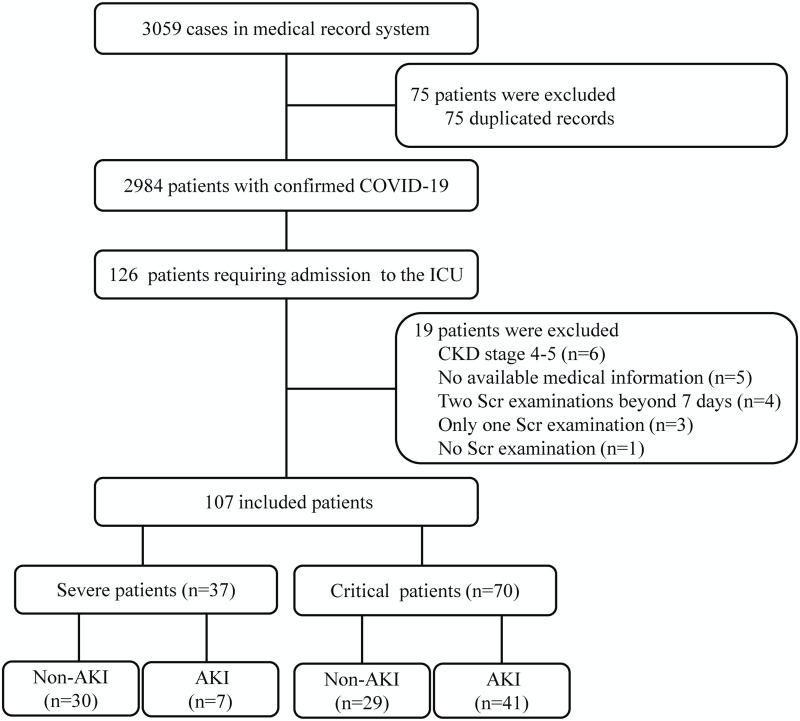
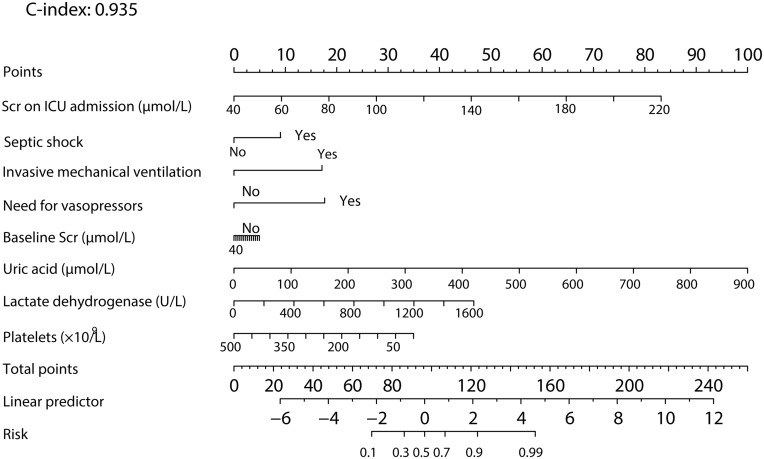
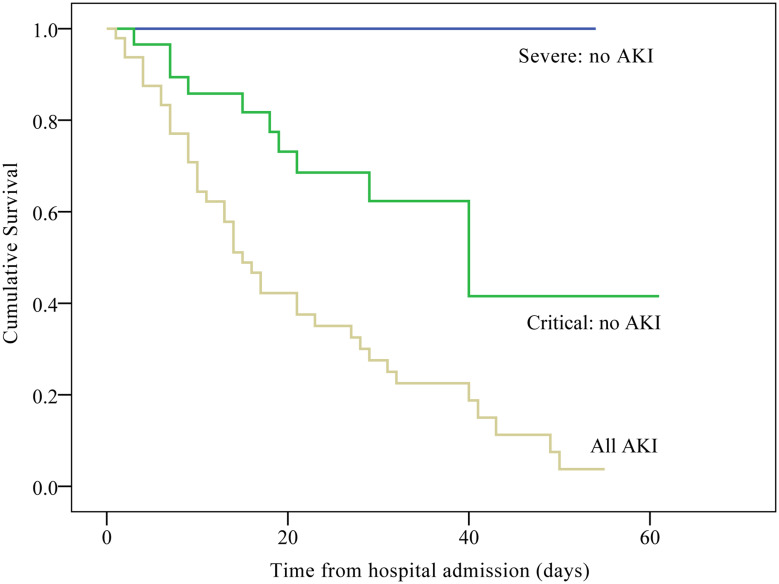
A total of 107 elderly patients were enrolled during the study period. The mean age was 70 (64-78) years, and 69 (64.5%) were men. For the 107 patients, the degree of severity of COVID-19 was categorized as 37 patients with the severe type (34.6%) and 70 patients with the critical type (65.4%). Overall, 48 of the 107 patients (44.9%) developed AKI during their hospitalization, while AKI occurred in 7 (18.9%) out of the 37 severe patients and 41 (44.9%) out of the 70 critical patients. Of the AKI patients, 35.4% (17/48) required continuous renal replacement therapy, including 14.3% of AKI patients in severe cases and 39.0% of AKI patients in critical cases. Kaplan-Meier analysis demonstrated that patients with AKI had a significantly higher risk for in-hospital mortality than severely and critically ill patients without AKI. Multivariate logistic regression analysis showed that AKI (OR = 33.74; 95% CI = 3.34-341.29; = 0.003), septic shock (OR = 15.58; 95% CI = 2.08-116.78; = 0.008), invasive mechanical ventilation (OR = 18.44; 95% CI = 2.35-144.69; = 0.006), and oxygenation index (OR = 0.99; 95% CI = 0.98-1.000; = 0.014) were independent risk factors for in-hospital mortality. A nomogram was established based on the multivariate analysis results. The C-index for the developed AKI model was 0.935 (95% CI, 0.892-0.978); when 10-fold cross validation was used to validate the model, the corrected C-index was 0.825.
AKI is common among COVID-19 patients admitted to the ICU and is recognized as a marker of disease severity. The proposed nomogram accurately predicted AKI development in ICU patients with COVID-19 based on individual characteristics. Therefore, the strategy for kidney protection against severe or critical pneumonia is appropriate.
患有 2019 年冠状病毒病(COVID-19)的重症或危重症患者发生急性肾损伤(AKI)的风险增加。然而,不同严重程度患者的 AKI 发生率以及与 AKI 相关的独立预测因素尚不清楚。
我们纳入了 107 例在中国武汉重症监护病房(ICU)住院的重症或危重症老年 COVID-19 患者。AKI 按照 2012 年 KDIGO 标准定义。我们使用逻辑回归探讨 AKI 与住院死亡率之间的关系。基于多变量逻辑回归制定预测 AKI 发生的列线图。
研究期间共纳入 107 例老年患者。平均年龄为 70(64-78)岁,69 例(64.5%)为男性。107 例患者中,COVID-19 的严重程度分为 37 例重症(34.6%)和 70 例危重症(65.4%)。总的来说,107 例患者中有 48 例(44.9%)在住院期间发生 AKI,其中 7 例(18.9%)重症患者和 41 例(44.9%)危重症患者发生 AKI。在 AKI 患者中,35.4%(17/48)需要持续肾脏替代治疗,包括 14.3%的重症 AKI 患者和 39.0%的危重症 AKI 患者。Kaplan-Meier 分析表明,与未发生 AKI 的重症和危重症患者相比,发生 AKI 的患者住院死亡率显著更高。多变量逻辑回归分析表明,AKI(OR=33.74;95%CI=3.34-341.29;P=0.003)、脓毒症休克(OR=15.58;95%CI=2.08-116.78;P=0.008)、有创机械通气(OR=18.44;95%CI=2.35-144.69;P=0.006)和氧合指数(OR=0.99;95%CI=0.98-1.000;P=0.014)是住院死亡率的独立危险因素。根据多变量分析结果建立了列线图。所开发的 AKI 模型的 C 指数为 0.935(95%CI,0.892-0.978);当使用 10 倍交叉验证来验证模型时,校正的 C 指数为 0.825。
AKI 在入住 ICU 的 COVID-19 患者中很常见,被认为是疾病严重程度的标志。所提出的列线图基于个体特征准确预测了 ICU 中 COVID-19 患者的 AKI 发生情况。因此,针对严重或危重症肺炎的肾脏保护策略是合适的。