Institute for Exercise and Environmental Medicine, Texas Health Presbyterian Hospital, Dallas (S.S., M.S., B.D.L.).
Department of Internal Medicine, University of Texas Southwestern Medical Center, Dallas (S.S., B.D.L.).
Circulation. 2021 Feb 23;143(8):783-789. doi: 10.1161/CIRCULATIONAHA.120.048338. Epub 2020 Nov 18.
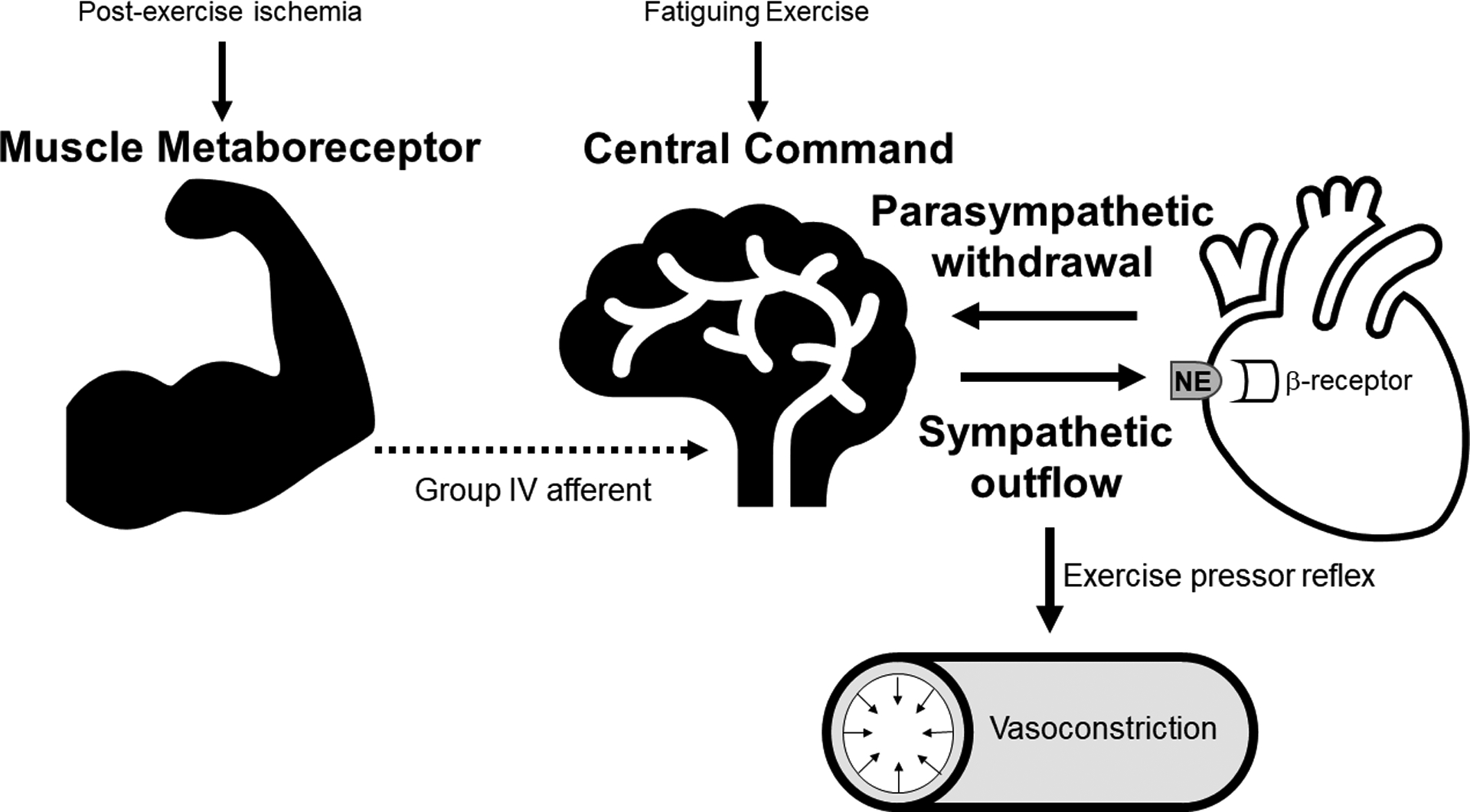
Chronotropic incompetence is common in heart failure with preserved ejection fraction (HFpEF) and is linked to impaired aerobic capacity. Whether upstream autonomic signaling pathways responsible for raising exercise heart rate are impaired in HFpEF is unknown. We investigated the integrity of central command and muscle metaboreceptor function, 2 predominant mechanisms responsible for exertional increases in heart rate, in patients with HFpEF and senior controls.
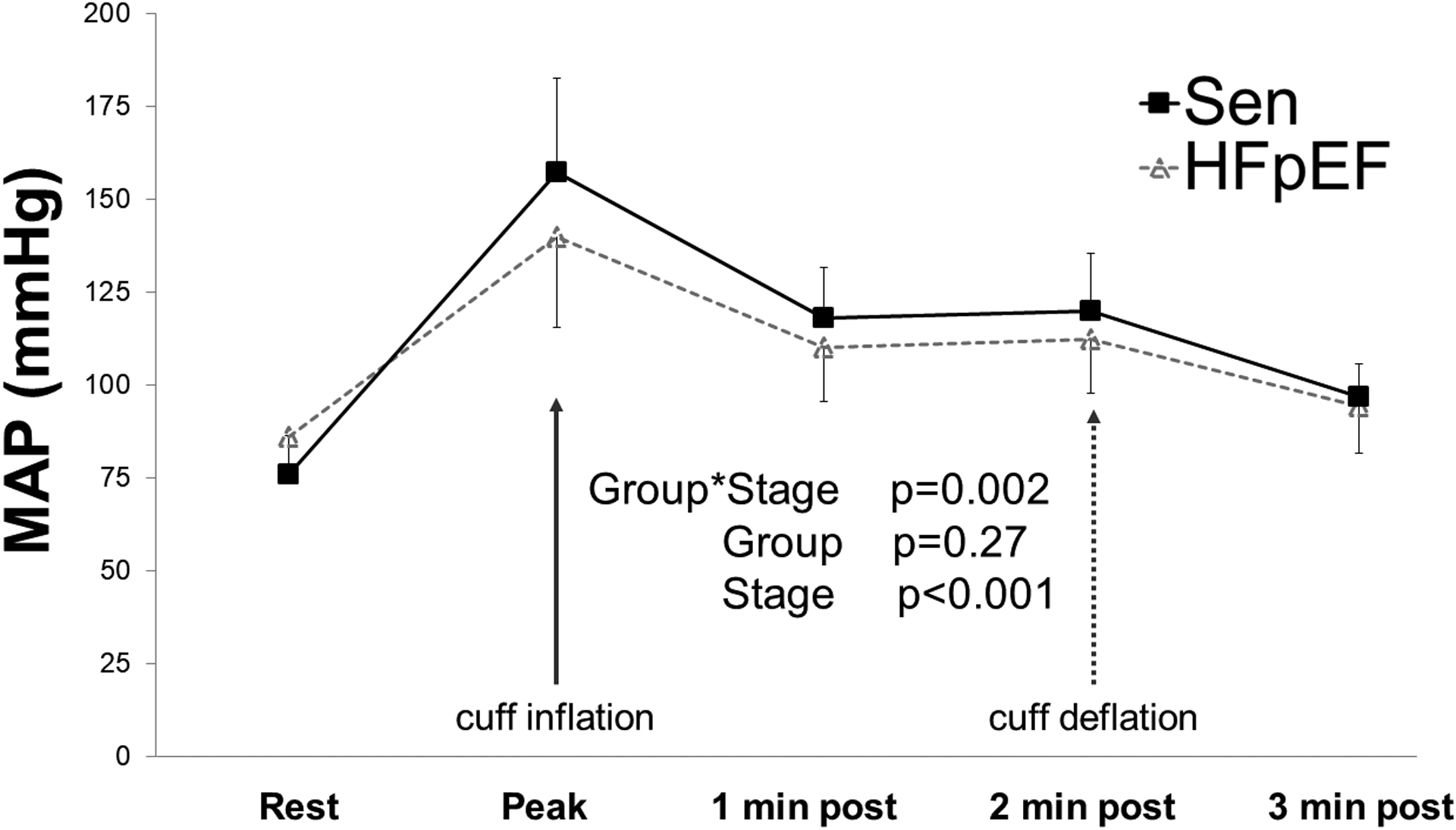
Fourteen healthy senior controls (7 men, 7 women) and 20 carefully screened patients with HFpEF (8 men, 12 women) underwent cardiopulmonary exercise testing (peak Vo) and static handgrip exercise at 40% of maximal voluntary contraction to fatigue with postexercise circulatory arrest for 2 minutes to assess central command and metaboreceptor function, respectively.
Peak Vo (13.1±3.4 versus 22.7±4.0 mL/kg/min; <0.001) and heart rate (122±20 versus 155±14 bpm; <0.001) were lower in patients with HFpEF than senior controls. There were no significant differences in peak heart rate response during static handgrip between groups (patients with HFpEF versus controls: 90±13 versus 93±10 bpm; =0.49). Metaboreceptor function, defined as mean arterial blood pressure at the end of postexercise circulatory arrest, was not significantly different between groups.
Central command (vagally mediated) and metaboreceptor function (sympathetically mediated) in patients with HFpEF were not different from those in healthy senior controls despite significantly lower peak whole-body exercise heart rates. These results demonstrate key reflex autonomic pathways regulating exercise heart rate responsiveness are intact in HFpEF.
在射血分数保留的心力衰竭(HFpEF)中,变时性功能不全很常见,并且与有氧运动能力受损有关。负责提高运动时心率的上游自主神经信号通路在 HFpEF 中是否受损尚不清楚。我们研究了 HFpEF 患者和老年对照组中负责运动时心率增加的中枢命令和肌肉代谢感受器功能的完整性,这是两个主要的机制。
14 名健康的老年对照组(7 名男性,7 名女性)和 20 名经过精心筛选的 HFpEF 患者(8 名男性,12 名女性)进行心肺运动测试(峰值 Vo)和 40%最大自主收缩的静态握力运动,直至疲劳,然后进行 2 分钟的运动后循环停止,以分别评估中枢命令和代谢感受器功能。
HFpEF 患者的峰值 Vo(13.1±3.4 与 22.7±4.0 mL/kg/min;<0.001)和心率(122±20 与 155±14 bpm;<0.001)均低于老年对照组。两组之间静态握力时的峰值心率反应没有显著差异(HFpEF 患者与对照组:90±13 与 93±10 bpm;=0.49)。运动后循环停止时的平均动脉血压定义的代谢感受器功能在两组之间没有显著差异。
尽管 HFpEF 患者的整体运动时心率明显较低,但 HFpEF 患者的中枢命令(迷走神经介导)和代谢感受器功能(交感神经介导)与健康老年对照组没有不同。这些结果表明,调节运动时心率反应的关键反射自主神经通路在 HFpEF 中是完整的。