Division of Cardiology Department of Internal Medicine University of Texas Southwestern Medical Center Dallas TX.
Institute for Exercise and Environmental Medicine Texas Health Presbyterian Hospital Dallas TX.
J Am Heart Assoc. 2020 Sep;9(17):e015794. doi: 10.1161/JAHA.120.015794. Epub 2020 Aug 27.
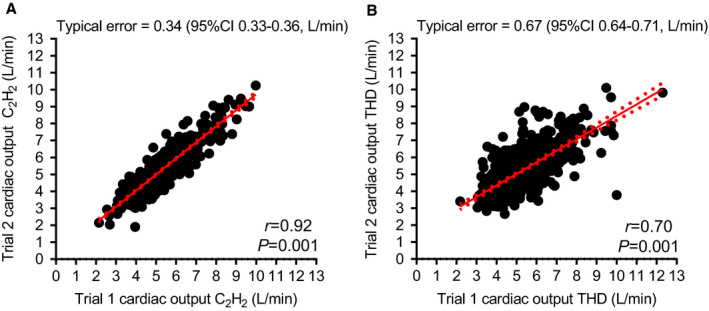
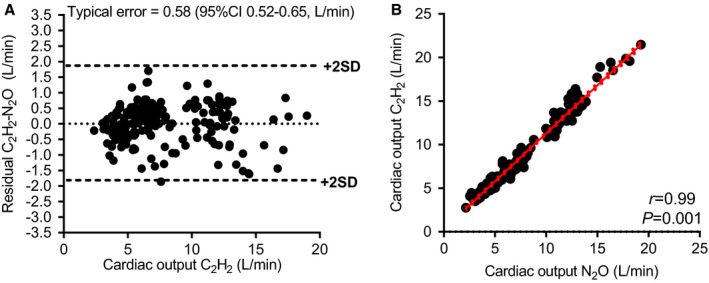
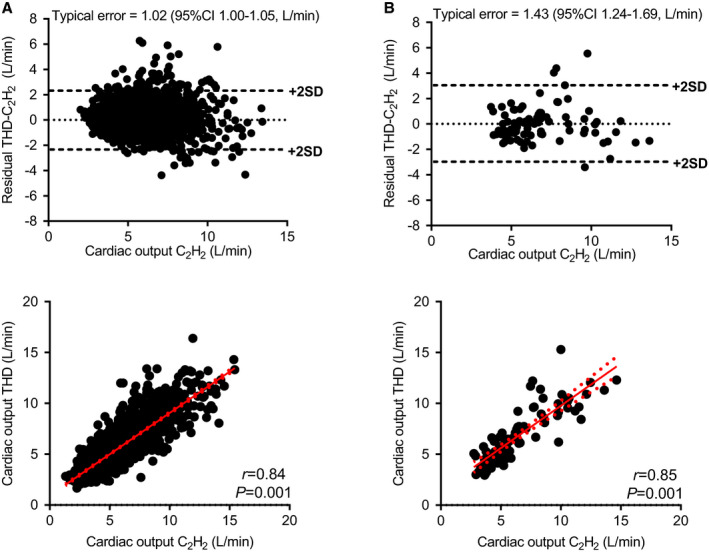
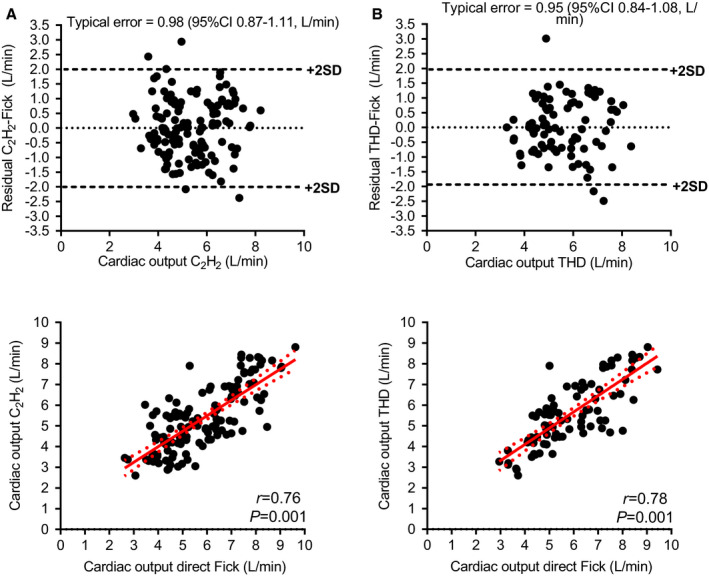
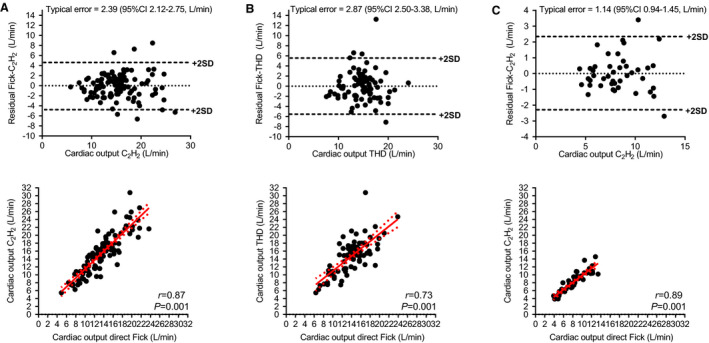
Background Accurate assessment of cardiac output is critical to the diagnosis and management of various cardiac disease states; however, clinical standards of direct Fick and thermodilution are invasive. Noninvasive alternatives, such as closed-circuit acetylene (CH) rebreathing, warrant validation. Methods and Results We analyzed 10 clinical studies and all available cardiopulmonary stress tests performed in our laboratory that included a rebreathing method and direct Fick or thermodilution. Studies included healthy individuals and patients with clinical disease. Simultaneous cardiac output measurements were obtained under normovolemic, hypovolemic, and hypervolemic conditions, along with submaximal and maximal exercise. A total of 3198 measurements in 519 patients were analyzed (mean age, 59 years; 48% women). The CH method was more precise than thermodilution in healthy individuals with half the typical error (TE; 0.34 L/min [=0.92] and coefficient of variation, 7.2%) versus thermodilution (TE=0.67 [=0.70] and coefficient of variation, 13.2%). In healthy individuals during supine rest and upright exercise, CH correlated well with thermodilution (supine: =0.84, TE=1.02; exercise: =0.82, TE=2.36). In patients with clinical disease during supine rest, CH correlated with thermodilution (=0.85, TE=1.43). CH was similar to thermodilution and nitrous oxide (NO) rebreathing technique compared with Fick in healthy adults (CH rest: =0.85, TE=0.84; CH exercise: =0.87, TE=2.39; thermodilution rest: =0.72, TE=1.11; thermodilution exercise: =0.73, TE=2.87; NO rest: =0.82, TE=0.94; NO exercise: =0.84, TE=2.18). The accuracy of the CH and NO methods was excellent (=0.99, TE=0.58). Conclusions The CH rebreathing method is more precise than, and as accurate as, the thermodilution method in a variety of patients, with accuracy similar to an NO rebreathing method approved by the US Food and Drug Administration.
准确评估心输出量对于各种心脏疾病的诊断和治疗至关重要;然而,直接 Fick 和热稀释法的临床标准是有创的。需要对非侵入性替代方法(如闭路乙炔(CH)再呼吸)进行验证。
我们分析了 10 项临床研究和我们实验室进行的所有可用心肺应激测试,其中包括再呼吸方法和直接 Fick 或热稀释法。研究包括健康个体和患有临床疾病的患者。在正常血容量、低血容量和高血容量条件下,以及亚最大和最大运动下,同时获得心输出量测量值。对 519 名患者的 3198 次测量值进行了分析(平均年龄 59 岁;48%为女性)。CH 方法在健康个体中比热稀释法更精确,其典型误差(TE)为 0.34L/min(=0.92),变异系数为 7.2%,而热稀释法的 TE 为 0.67(=0.70),变异系数为 13.2%。在健康个体仰卧休息和直立运动期间,CH 与热稀释法相关性良好(仰卧:=0.84,TE=1.02;运动:=0.82,TE=2.36)。在患有临床疾病的患者仰卧休息时,CH 与热稀释法相关(=0.85,TE=1.43)。CH 与热稀释法和一氧化二氮(NO)再呼吸技术与健康成年人的 Fick 法相似(CH 休息:=0.85,TE=0.84;CH 运动:=0.87,TE=2.39;热稀释休息:=0.72,TE=1.11;热稀释运动:=0.73,TE=2.87;NO 休息:=0.82,TE=0.94;NO 运动:=0.84,TE=2.18)。CH 和 NO 方法的准确性极好(=0.99,TE=0.58)。
CH 再呼吸法在各种患者中比热稀释法更精确,且准确性与经美国食品和药物管理局批准的 NO 再呼吸法相似。