Shin Sumin, Kang Danbee, Cho Jong Ho, Choi Yong Soo, Kim Jhingook, Zo Jae Ill, Shim Young Mog, Kim Hong Kwan
Department of Thoracic and Cardiovascular Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
Department of Clinical Research Design & Evaluation, Samsung Advanced Institute for Health Sciences & Technology (SAIHST), Sungkyunkwan University, Seoul, Korea.
J Thorac Dis. 2020 Oct;12(10):5552-5560. doi: 10.21037/jtd-20-1611.
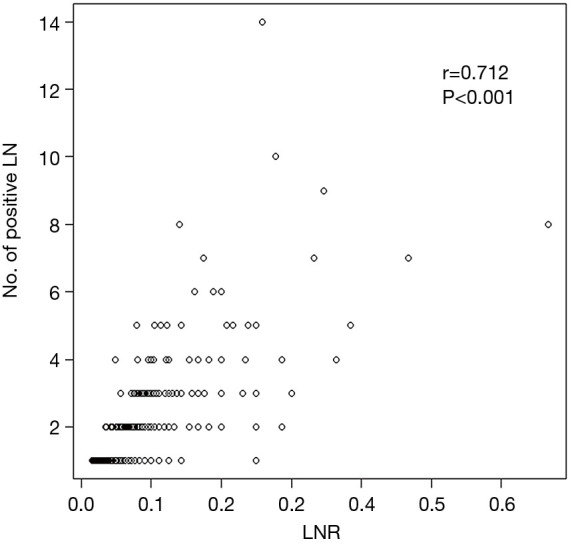
This study evaluated the lymph node ratio (LNR) defined as the ratio of the number of metastatic lymph nodes to the number of dissected lymph nodes as a prognostic factor for survival in patients with pT1-2N1M0 non-small cell lung cancer (NSCLC).
We retrospectively reviewed 413 patients with pathologic T1-2N1M0 NSCLC after complete surgical resection and mediastinal LN dissection between January 2004 and December 2012. The cut-off value for LNR was determined using χ tests, which were calculated using Cox proportional hazards regression model. Based on this model, the optimal cut-off value for LNR was 0.1.
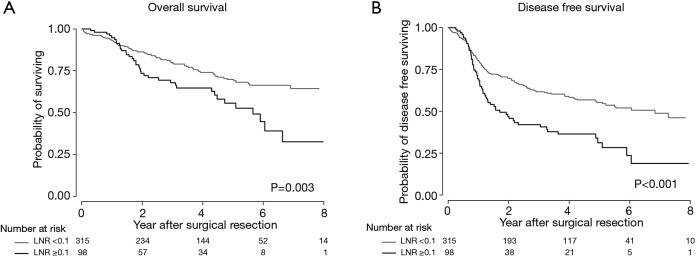
The study included 337 males and 76 females with a mean age of 62 years (range, 34-83 years). Patients with a high LNR (≥0.1) were more likely to be female and have more adenocarcinomas compared with patients with a low LNR (<0.1). The overall survival (OS) and disease-free survival (DFS) rates were significantly worse in the high LNR group than the low LNR group (OS, 55.4% 69.8%, respectively P=0.003; DFS, 33.2% 61.7%, P<0.001). In the multivariate analysis, a high LNR was associated with significantly worse OS [adjusted hazard ratio (aHR), 2.69; 95% confidence interval (CI), 1.74-4.17] and DFS (aHR, 2.41; 95% CI, 1.57-3.68).
LNR is an independent prognostic factor for survival in patients with pT1-2N1M0 NSCLC. These findings may provide useful prognostic information to allow the selection of patients for more aggressive postoperative therapy or follow-up strategies.
本研究评估了淋巴结比率(LNR),即转移淋巴结数量与清扫淋巴结数量之比,作为pT1-2N1M0非小细胞肺癌(NSCLC)患者生存的预后因素。
我们回顾性分析了2004年1月至2012年12月间413例行完全手术切除及纵隔淋巴结清扫的病理T1-2N1M0 NSCLC患者。LNR的临界值采用χ检验确定,通过Cox比例风险回归模型计算得出。基于该模型,LNR的最佳临界值为0.1。
本研究纳入337例男性和76例女性,平均年龄62岁(范围34-83岁)。与LNR低(<0.1)的患者相比,LNR高(≥0.1)的患者更可能为女性且腺癌更多。高LNR组的总生存(OS)率和无病生存(DFS)率显著低于低LNR组(OS分别为55.4%和69.8%,P=0.003;DFS分别为33.2%和61.7%,P<0.001)。多因素分析中,高LNR与显著更差的OS(调整后风险比[aHR],2.69;95%置信区间[CI],1.74-4.17)和DFS(aHR,2.41;95%CI,1.57-3.68)相关。
LNR是pT1-2N1M0 NSCLC患者生存的独立预后因素。这些发现可能为选择更积极的术后治疗或随访策略的患者提供有用的预后信息。