Sangaré Mohamed N'dongo, Baril Jean-Guy, de Pokomandy Alexandra, Laprise Claudie, Deshaies Catherine, Klein Marina, Thomas Réjean, Tremblay Cécile, Roger Michel, Pexos Costa, Greenwald Zoe, Machouf Nima, Durand Madeleine, Hardy Isabelle, Dakouo Mamadou, Laporte Louise, Trottier Helen
Department of Social and Preventive Medicine, Université de Montréal.
Sainte Justine University Hospital Center.
Medicine (Baltimore). 2020 Nov 20;99(47):e23335. doi: 10.1097/MD.0000000000023335.
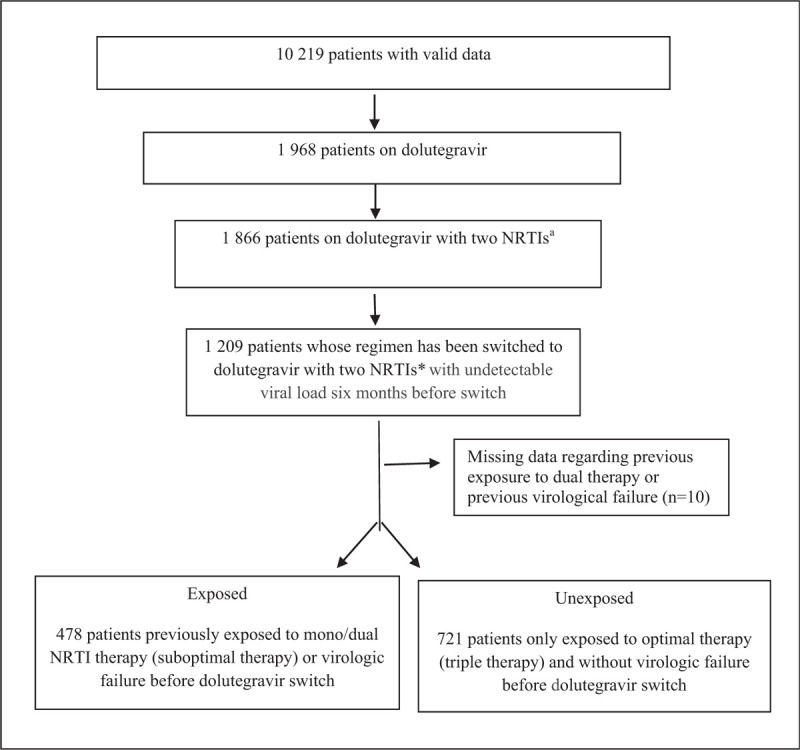
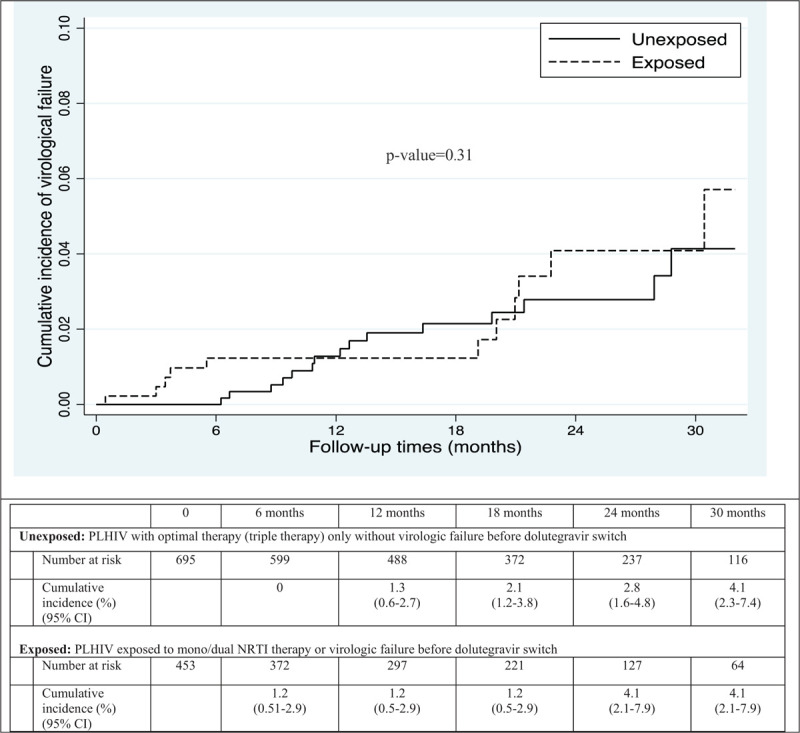
There is uncertainty regarding the potential virologic outcome associated with a change in antiretroviral therapy (ARV) among PLHIV who had previous documented virologic failure or who have been exposure to mono/dual nucleoside reverse transcriptase inhibitors (NRTI) therapy. The objective was to measure the potential impact of exposure to previous virologic failure or mono/dual NRTI regimen on virologic outcome of PLHIV following a switch to dolutegravir with 2 NRTIs from a viremia suppressive ARV therapy.Data from the Quebec HIV Cohort including 10219 PLHIV were collected through routine clinical care at 4 clinical sites in Montreal, Canada. This study includes patients whose ARV therapy was switched to dolutegravir with 2 NRTIs since 2013 with undetectable viral load for ≥6 months before switch. The association between exposure and post-switch virologic outcome was measured by marginal hazard ratio estimated using the Inverse probability weighting Cox model.Among the 1199 eligible PLHIV, 478 (39.9%) previously experienced at least one virologic failure or were exposed to mono/dual therapy before dolutegravir switch. Post-switch virologic failure after 30 months occurred in 4.1% (95% CI 2.1-7.9) of exposed compared to 4.1% (95% CI 2.3-7.4) in unexposed participants. The adjusted hazard ratio for the association between exposure and post-switch virologic failure was 0.84 (95% CI 0.35-2.01).Our findings suggest that switch to dolutegravir with 2 NRTIs from a suppressive therapy is a safe option for PLHIV with documented virologic failure and/or previous exposure to mono/dual NRTI therapy.
对于既往有病毒学失败记录或曾接受单/双核苷类逆转录酶抑制剂(NRTI)治疗的艾滋病毒感染者(PLHIV),改变抗逆转录病毒疗法(ARV)后的潜在病毒学结果存在不确定性。目的是衡量既往病毒学失败或单/双NRTI治疗方案对PLHIV从病毒血症抑制性ARV疗法转换为多替拉韦加两种NRTI后的病毒学结果的潜在影响。通过加拿大蒙特利尔4个临床地点的常规临床护理收集了来自魁北克艾滋病毒队列的10219名PLHIV的数据。本研究包括自2013年以来ARV疗法转换为多替拉韦加两种NRTI且转换前病毒载量至少6个月检测不到的患者。暴露与转换后病毒学结果之间的关联通过使用逆概率加权Cox模型估计的边际风险比来衡量。在1199名符合条件的PLHIV中,478名(39.9%)在转换多替拉韦之前曾经历至少一次病毒学失败或接受过单/双疗法。转换后30个月时,暴露组的病毒学失败发生率为4.1%(95%CI 2.1 - 7.9),未暴露组为4.1%(95%CI 2.3 - 7.4)。暴露与转换后病毒学失败之间关联的调整后风险比为0.84(95%CI 0.35 - 2.01)。我们的研究结果表明,对于有病毒学失败记录和/或既往接受过单/双NRTI治疗的PLHIV,从抑制性疗法转换为多替拉韦加两种NRTI是一种安全的选择。