Gurney Jason, Stanley James, Sarfati Diana
Cancer and Chronic Conditions (C3) Research Group, Department of Public Health, University of Otago, Wellington, New Zealand.
Cancer Control Agency, Wellington, New Zealand.
J Comorb. 2020 Nov 10;10:2235042X20971168. doi: 10.1177/2235042X20971168. eCollection 2020 Jan-Dec.
The burden of chronic disease is not evenly shared within our society. In this manuscript, we use comprehensive national-level data to compare morbidity burden between ethnic groups in New Zealand.
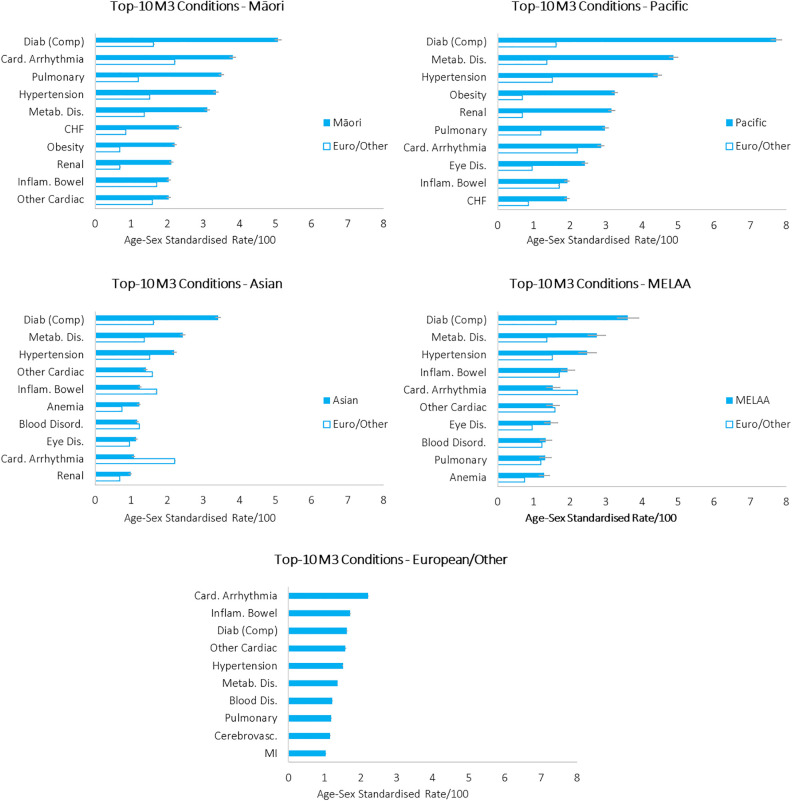
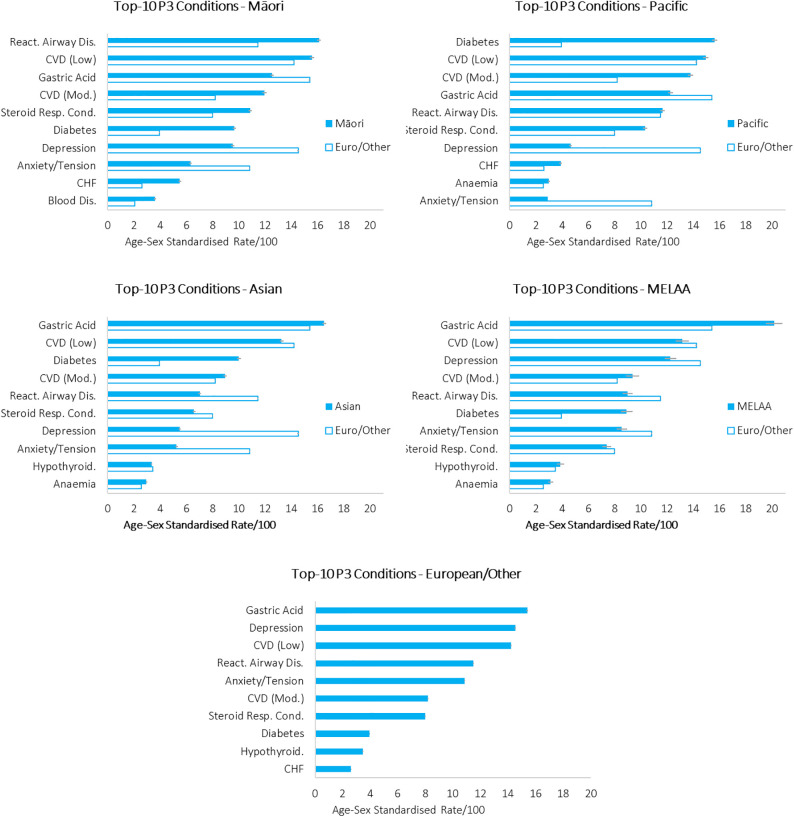
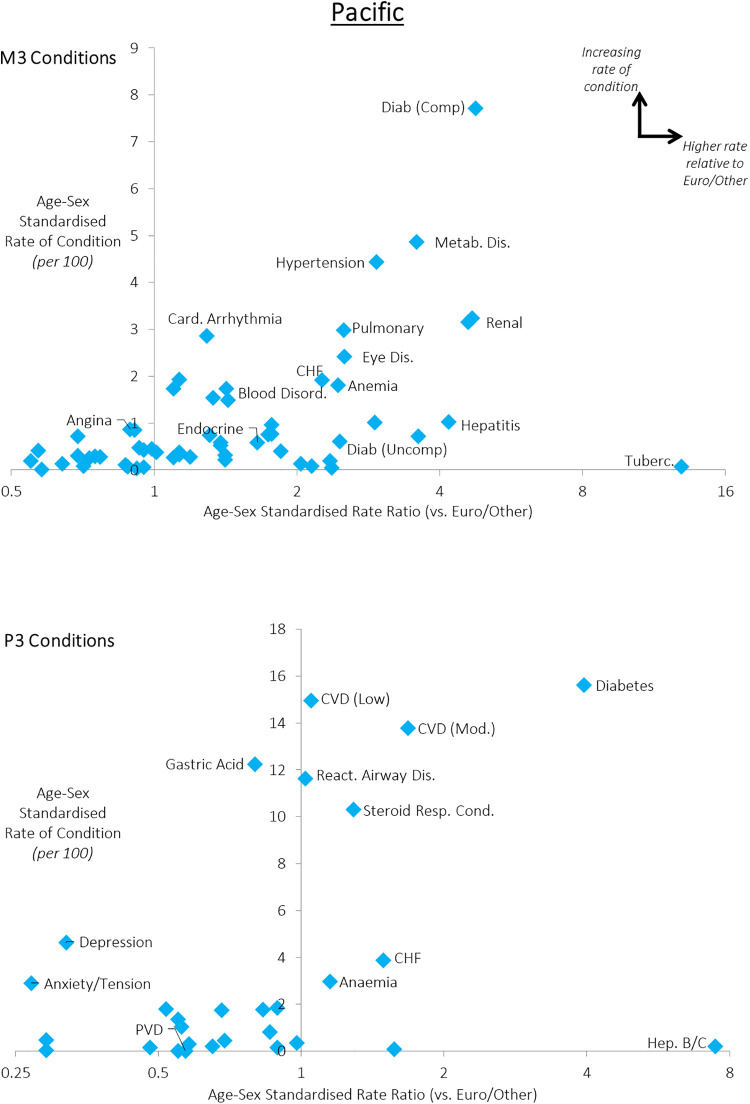
We investigated the prevalence of morbidity among all New Zealanders aged 18+ (n = 3,296,837), stratified by ethnic group (Māori, Pacific, Asian, Middle Eastern/Latin American/African, European/Other), using national-level hospitalisation and pharmaceutical data and two measures of morbidity (the M3 and P3 indices).
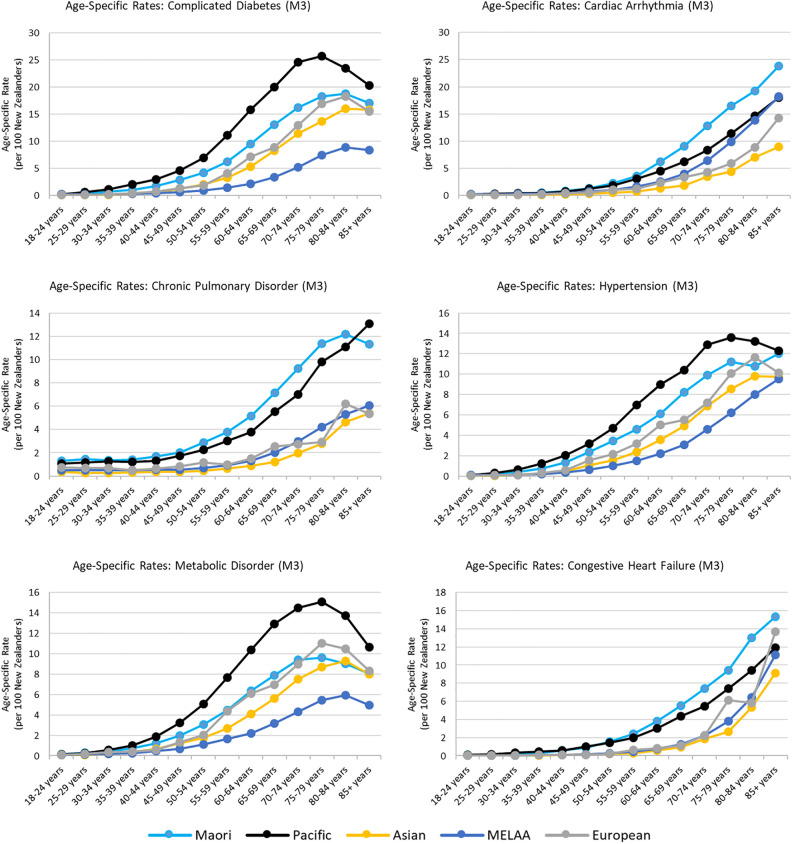
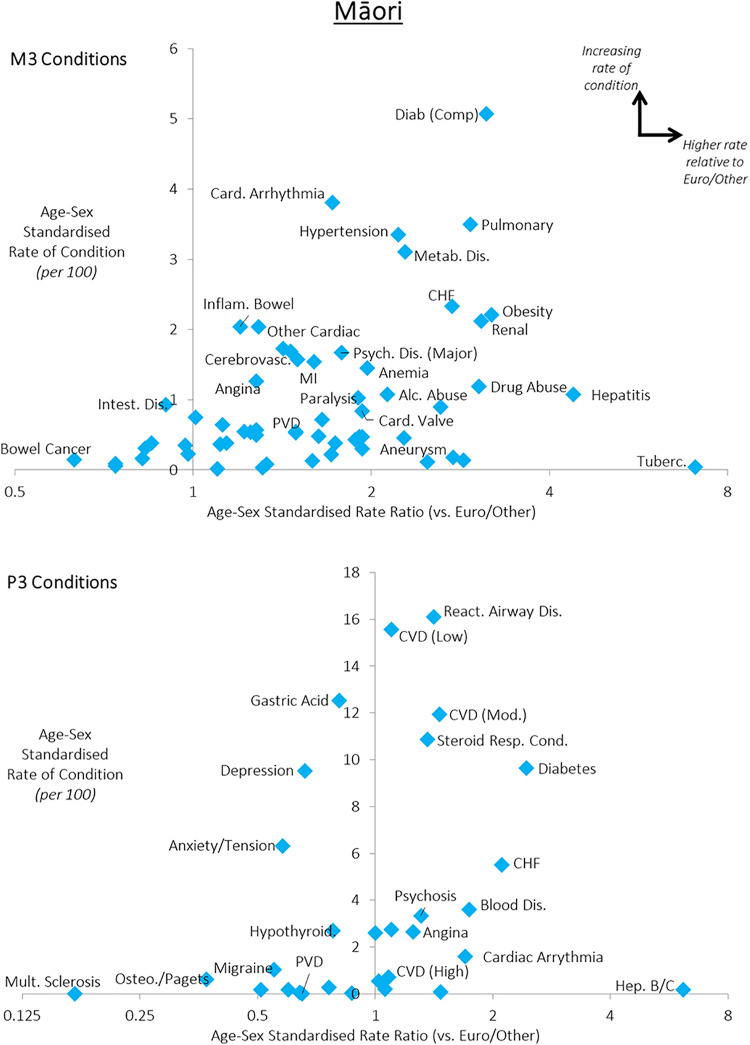
We observed substantial disparities for Māori and Pacific peoples compared to other ethnic groups for the vast majority of commonly-diagnosed morbidities. These disparities appeared strongest for the most-common conditions - meaning that Māori and Pacific peoples disproportionately shoulder an increased burden of these key conditions. We also observed that prevalence of these conditions emerged at earlier ages, meaning that Māori and Pacific peoples also experience a disproportionate impact of individual conditions on the quality and quantity of life. Finally, we observed strong disparities in the prevalence of conditions that may exacerbate the impact of COVID-19, such as chronic pulmonary, liver or renal disease. The substantial inequities we have presented here have been created and perpetuated by the social determinants of health, including institutionalised racism: thus solutions will require addressing these systemic issues as well as addressing inequities in individual-level care.
慢性病负担在我们的社会中并非平均分配。在本论文中,我们使用全面的国家级数据来比较新西兰不同种族之间的发病负担。
我们利用国家级住院和药物数据以及两种发病衡量指标(M3和P3指数),对所有18岁及以上的新西兰人(n = 3,296,837)按种族(毛利人、太平洋岛民、亚洲人、中东/拉丁美洲/非洲人、欧洲人/其他)进行分层,调查发病率。
与其他种族相比,我们观察到毛利人和太平洋岛民在绝大多数常见诊断疾病方面存在显著差异。这些差异在最常见的疾病中最为明显——这意味着毛利人和太平洋岛民不成比例地承担了这些关键疾病增加的负担。我们还观察到这些疾病的患病率在较早年龄就出现了,这意味着毛利人和太平洋岛民在个体疾病对生活质量和寿命的影响方面也受到了不成比例的影响。最后,我们观察到在可能加剧COVID-19影响的疾病患病率方面存在强烈差异,如慢性肺病、肝病或肾病。我们在此呈现的严重不平等是由健康的社会决定因素造成并长期存在的,包括制度化的种族主义:因此,解决方案需要解决这些系统性问题以及个体层面护理中的不平等问题。