Collonnaz Magali, Erpelding Marie-Line, Alla François, Goehringer François, Delahaye François, Iung Bernard, Le Moing Vincent, Hoen Bruno, Selton-Suty Christine, Agrinier Nelly
CHRU-Nancy, INSERM, CIC-EC, Epidémiologie clinique, F-54000 Nancy, France.
Université de Lorraine, APEMAC, F-54000 Nancy, France.
Data Brief. 2020 Nov 1;33:106478. doi: 10.1016/j.dib.2020.106478. eCollection 2020 Dec.
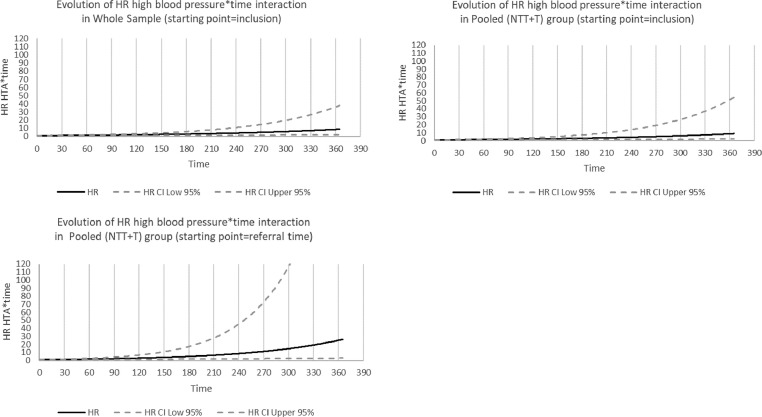
This article describes supplementary tables and figures associated with the research paper entitled "Impact of referral bias on prognostic studies outcomes: insights from a population-based cohort study on infective endocarditis". The aforementioned paper is a secondary analysis of data from the cohort on infective endocarditis and aimed at characterising referral bias. A total of 497 patients diagnosed with definite infective endocarditis between January 1 and December 31 2008 were included in . Data were collected from hospital medical records by trained clinical research assistants. Patients were divided into three groups: admitted to a tertiary hospital (group T), admitted to a non-tertiary hospital and referred secondarily to a tertiary hospital (group NTT) or admitted to a non-tertiary hospital and not referred (group NT). The pooled (NTT+T) group mimicked studies recruiting patients in tertiary hospitals only. Two different starting points were considered for follow up: date of first hospital admission and date of first admission to a tertiary hospital if any (hereinafter referred to as "referral time"). Referral bias is a type of selection bias which can occur due to recruitment of patients in tertiary hospitals only (excluding those who are admitted to non-tertiary hospitals and not referred to tertiary hospitals). This bias may impact the description of patients' characteristics, survival estimates as well as prognostic factors identification. The six tables presented in this paper illustrate how patients' selection (population-based sample [pooled (NT+NTT+T) group] versus recruitment in tertiary hospitals only [pooled (NTT+T) group]) might impact Hazards Ratios values for prognostic factors. Crude and adjusted Cox regression analyses were first performed to identify prognostic factors associated with 3-month and 1-year mortality in the whole sample using inclusion as the starting point. Analyses were then performed in the pooled (NTT+T) group first using inclusion as the starting point and finally using referral time as the starting point. Figures 1 to 3 illustrate how HR increase with time for covariates that were considered as time-varying covariates (covariate*time interaction).
本文介绍了与题为《转诊偏倚对预后研究结果的影响:基于人群的感染性心内膜炎队列研究的见解》的研究论文相关的补充表格和图表。上述论文是对感染性心内膜炎队列数据的二次分析,旨在描述转诊偏倚。2008年1月1日至12月31日期间共纳入497例确诊为明确感染性心内膜炎的患者。数据由经过培训的临床研究助理从医院病历中收集。患者分为三组:入住三级医院(T组)、入住非三级医院并二次转诊至三级医院(NTT组)或入住非三级医院且未转诊(NT组)。合并(NTT+T)组模拟了仅在三级医院招募患者的研究。随访考虑了两个不同的起始点:首次入院日期以及首次入住三级医院的日期(如有,以下简称“转诊时间”)。转诊偏倚是一种选择偏倚,可能由于仅在三级医院招募患者(排除那些入住非三级医院且未转诊至三级医院的患者)而发生。这种偏倚可能会影响患者特征的描述、生存估计以及预后因素的识别。本文呈现 的六个表格说明了患者选择(基于人群的样本[合并(NT+NTT+T)组]与仅在三级医院招募[合并(NTT+T)组])如何可能影响预后因素的风险比 值。首先进行粗 Cox 回归分析和校正 Cox 回归分析,以确定以纳入为起始点的整个样本中与3个月和1年死亡率相关的预后因素。然后首先在合并(NTT+T)组中以纳入为起始点进行分析,最后以转诊时间为起始点进行分析。图1至3说明了作为随时间变化的协变量(协变量*时间交互作用)的协变量的HR如何随时间增加。