Technology Enterprise Facility, Canadian Institute for Substance Use Research, University of Victoria, PO Box 1700 STN CSC, Victoria, BC, V8W 2Y2, Canada.
School of Public Health and Social Policy, University of Victoria, PO Box 1700 STN CSC, Victoria, BC, V8W 2Y2, Canada.
BMC Health Serv Res. 2020 Nov 23;20(1):1060. doi: 10.1186/s12913-020-05915-x.
People who use substances experience high levels of substance-related stigma, both within and outside of health care settings, which can prevent people from help-seeking and contribute further to health inequities. Recognizing and respecting how political, social, economic, and historical conditions influence health and health care, cultural safety, with origins in addressing Indigenous racism, is a potential strategy for mitigating stigma and marginalization in health care. Using a participatory research approach, we applied the concept of cultural safety to develop a model of safe primary care from the perspective of people who use substances.
People who use or used substances were involved in all phases of the research and led data collection. Study participants (n = 75) were 42.5 years old on average; half identified as female and one quarter as Indigenous. All were currently using or had previous experience with substances (alcohol and/or other drugs) and were recruited through two local peer-run support agencies. Concept mapping with hierarchical cluster analysis was used to develop the model of safe primary care, with data collected over three rounds of focus groups.
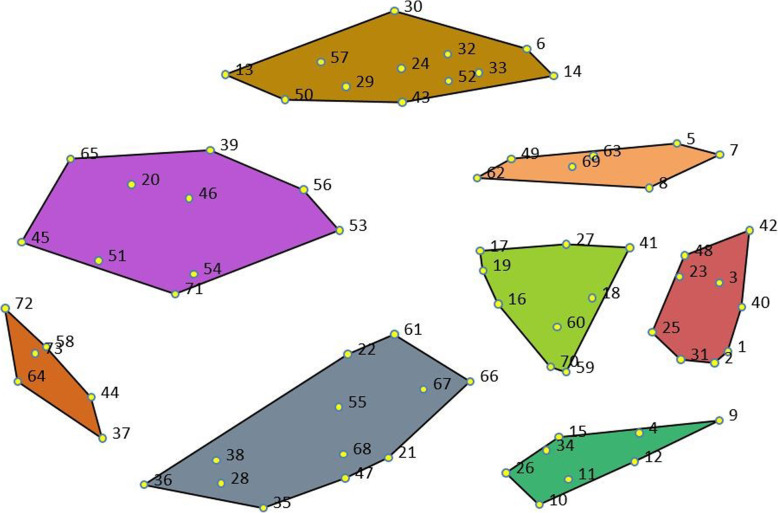
Participants identified 73 unique statements to complete the focus prompt: "I would feel safe going to the doctor if …" The final model consisted of 8 clusters that cover a wide range of topics, from being treated with respect and not being red-flagged for substance use, to preserving confidentiality, advocacy for good care and systems change, and appropriate accommodations for anxiety and the effects of poverty and criminalization.
Developing a definition of safe care (from the patient perspective) is the necessary first step in creating space for positive interactions and, in turn, improve care processes. This model provides numerous concrete suggestions for providers, as well as serving as starting point for the development of interventions designed to foster system change.
在医疗保健环境内外,使用物质的人都会经历高度的与物质相关的污名化,这可能会阻止人们寻求帮助,并进一步导致健康不平等。认识到并尊重政治、社会、经济和历史条件如何影响健康和医疗保健,文化安全(起源于解决土著种族主义问题)是减轻医疗保健中污名化和边缘化的潜在策略。我们采用参与式研究方法,从使用物质者的角度应用文化安全概念,制定了一个安全初级保健模型。
使用物质者参与了研究的所有阶段,并主导了数据收集。研究参与者(n=75)的平均年龄为 42.5 岁;一半为女性,四分之一为土著。所有人都目前正在使用或以前有过物质(酒精和/或其他药物)使用经验,并通过两个当地的同行支持机构招募。使用概念映射和层次聚类分析来开发安全初级保健模型,在三轮焦点小组中收集数据。
参与者共提出了 73 个独特的陈述来完成焦点提示:“如果……我去看医生会感到安全。”最终模型由 8 个集群组成,涵盖了广泛的主题,从受到尊重而不因药物使用而被标记,到保护隐私、倡导良好的护理和系统变革,以及适当考虑焦虑和贫困以及刑事定罪的影响。
从患者的角度出发,定义安全护理(定义)是为积极互动创造空间的必要的第一步,从而改善护理过程。该模型为提供者提供了许多具体建议,同时也为旨在促进系统变革的干预措施的发展提供了起点。