Haslett Kate, Bayman Neil, Franks Kevin, Groom Nicki, Harden Susan V, Harris Catherine, Hanna Gerard, Harrow Stephen, Hatton Matthew, McCloskey Paula, McDonald Fiona, Ryder W David, Faivre-Finn Corinne
The Christie NHS Foundation Trust Wilmslow Road, Manchester, United Kingdom; Department of Radiotherapy Related Research, University of Manchester, Manchester, United Kingdom.
The Christie NHS Foundation Trust Wilmslow Road, Manchester, United Kingdom.
Int J Radiat Oncol Biol Phys. 2021 Apr 1;109(5):1341-1348. doi: 10.1016/j.ijrobp.2020.11.040. Epub 2020 Nov 21.
Not all patients with stage III non-small cell lung cancer (NSCLC) are suitable for concurrent chemoradiation therapy (CRT). Local failure rate is high for sequential concurrent CRT. As such, there is a rationale for treatment intensification.
Isotoxic intensity modulated radiation therapy (IMRT) is a multicenter feasibility study that combines different intensification strategies including hyperfractionation, acceleration, and dose escalation facilitated by IMRT. Patients with unresectable stage III NSCLC, Eastern Cooperative Oncology Group (ECOG) performance status (PS) of 0 to 2, and unsuitable for concurrent CRT were recruited. A minimum of 2 cycles of platinum-based chemotherapy was compulsory before starting radiation therapy (RT). Radiation dose was increased until a maximum dose of 79.2 Gy was reached or 1 or more of the organs at risk met predefined constraints. RT was delivered in 1.8-Gy fractions twice daily, and an RT quality assurance program was implemented. The primary objective was the delivery of isotoxic IMRT to a dose >60 Gy equivalent dose in 2-Gy fractions (EQD2 assuming an α/β ratio of 10 Gy for acute reacting tissues).
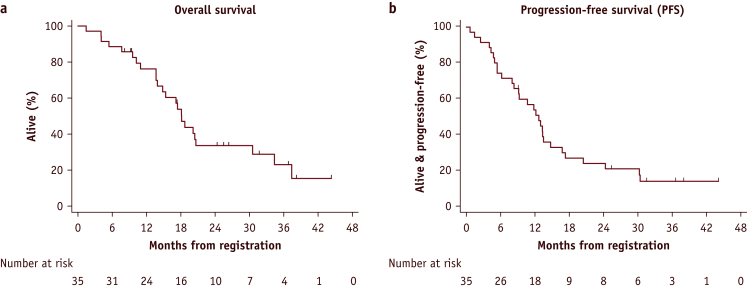
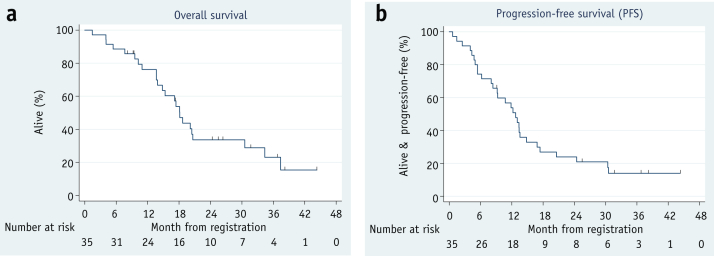
Thirty-seven patients were recruited from 7 UK centers. Median age was 69.9 years (range, 46-86 years). The male-to-female ratio was 17:18. ECOG PS was 0 to 5 in 14.2% of patients; PS was 1 to 27 in 77.1% of patients; PS was 2 to 3 in 8.6% of patients. Stage IIIA:IIIB ratio was 22:13 (62.9%:37.1%). Of 37 patients, 2 (5.4%) failed to achieve EQD2 > 60 Gy. Median prescribed tumor dose was 77.4 Gy (range, 61.2-79.2 Gy). A maximum dose of 79.2Gy was achieved in 14 patients (37.8%). Grade 3 esophagitis was reported in 2 patients, and no patients developed grade 3 to 4 pneumonitis. There were 3 grade 5 events: acute radiation pneumonitis, bronchopulmonary hemorrhage, and acute lung infection. Median follow-up at time of analysis was 25.4 months (range, 8.0-44.2) months for 11 of 35 survivors. The median survival was 18.1 months (95% confidence interval [CI], 13.9-30.6), 2-year overall survival was 33.6% (95% CI, 17.9-50.1), and progression-free survival was 23.9% (95% CI, 11.3-39.1).
Isotoxic IMRT is a well-tolerated and feasible approach to treatment intensification.
并非所有Ⅲ期非小细胞肺癌(NSCLC)患者都适合同步放化疗(CRT)。序贯同步CRT的局部失败率较高。因此,有理由加强治疗。
等毒性调强放射治疗(IMRT)是一项多中心可行性研究,结合了不同的强化策略,包括超分割、加速和通过IMRT实现的剂量递增。招募了无法切除的Ⅲ期NSCLC患者,东部肿瘤协作组(ECOG)体能状态(PS)为0至2且不适合同步CRT的患者。在开始放射治疗(RT)前至少进行2个周期的铂类化疗是强制性的。放射剂量增加直至达到最大剂量79.2 Gy或1个或更多危及器官达到预定义的限制。RT以1.8 Gy的分次剂量每天两次给予,并实施了RT质量保证计划。主要目标是给予等毒性IMRT至剂量>60 Gy等效剂量(2 Gy分次剂量,假设急性反应组织的α/β比值为10 Gy时的等效剂量[EQD2])。
从7个英国中心招募了37例患者。中位年龄为69.9岁(范围46 - 86岁)。男女比例为17:18。14.2%的患者ECOG PS为0至1;77.1%的患者PS为1至2;8.6%的患者PS为2至3。ⅢA期:ⅢB期比例为22:13(62.9%:37.1%)。37例患者中,2例(5.4%)未达到EQD2>60 Gy。中位规定肿瘤剂量为77.4 Gy(范围61.2 - 79.2 Gy)。14例患者(37.8%)达到最大剂量79.2 Gy。2例患者报告有3级食管炎,无患者发生3至4级肺炎。有3例5级事件:急性放射性肺炎、支气管肺出血和急性肺部感染。分析时35例幸存者中11例的中位随访时间为25.4个月(范围8.0 - 44.2个月)。中位生存期为18.1个月(95%置信区间[CI],13.9 - 30.6),2年总生存率为33.6%(95% CI,17.9 - 50.1),无进展生存率为23.9%(95% CI,11.3 - 39.1)。
等毒性IMRT是一种耐受性良好且可行的强化治疗方法。