Streng Alexander S, Delnoij Thijs S R, Mulder Mark M G, Sels Jan Willem E M, Wetzels Rick J H, Verhezen Paul W M, Olie Renske H, Kooman Jeroen P, van Kuijk Sander M J, Brandts Lloyd, Ten Cate Hugo, Lorusso Roberto, van der Horst Iwan C C, van Bussel Bas C T, Henskens Yvonne M C
Central Diagnostic Laboratory, Maastricht University Medical Centre, Maastricht, the Netherlands.
Intensive Care Unit, Maastricht University Medical Centre, Maastricht, the Netherlands.
TH Open. 2020 Nov 19;4(4):e365-e375. doi: 10.1055/s-0040-1719083. eCollection 2020 Oct.
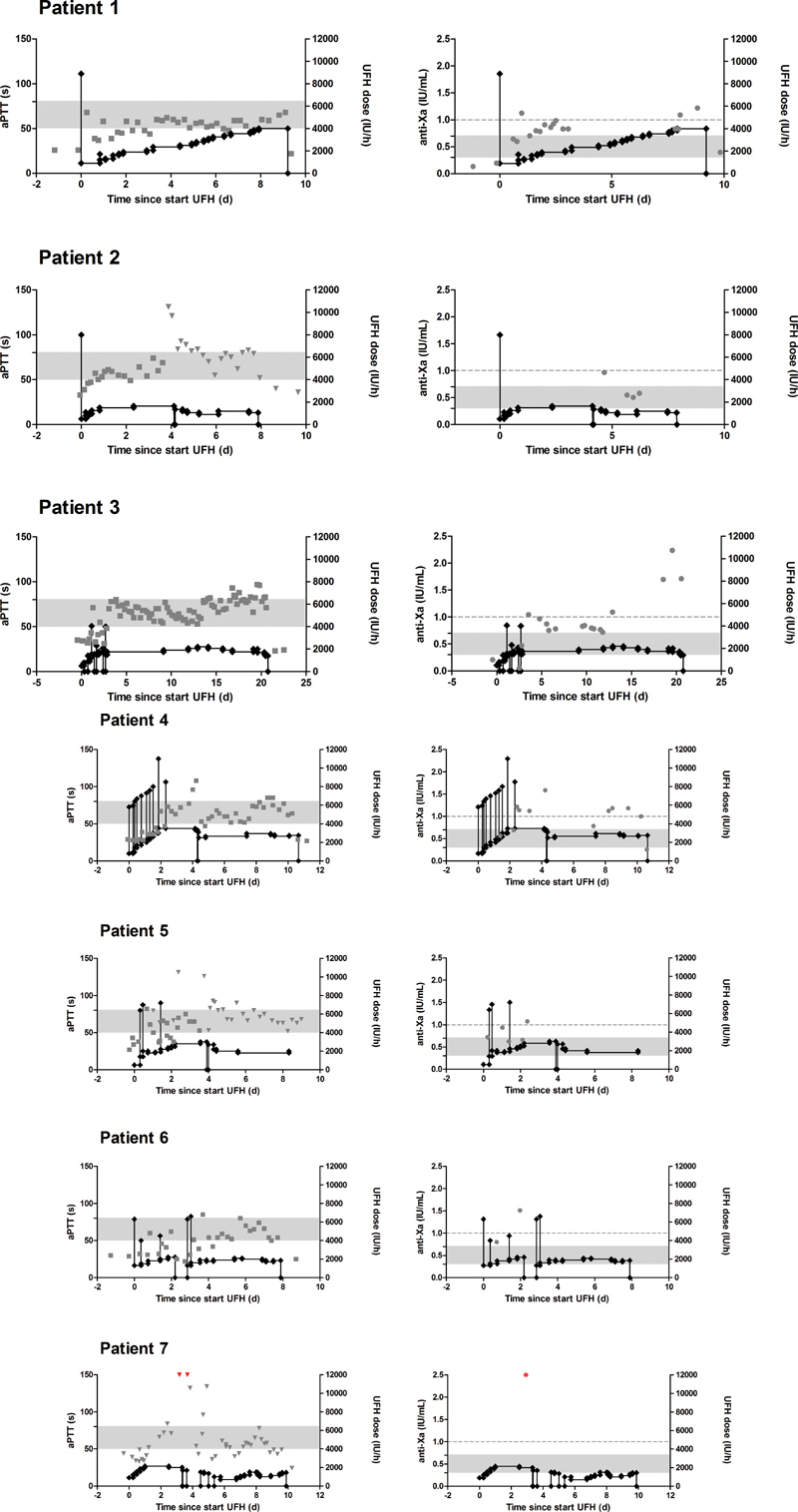
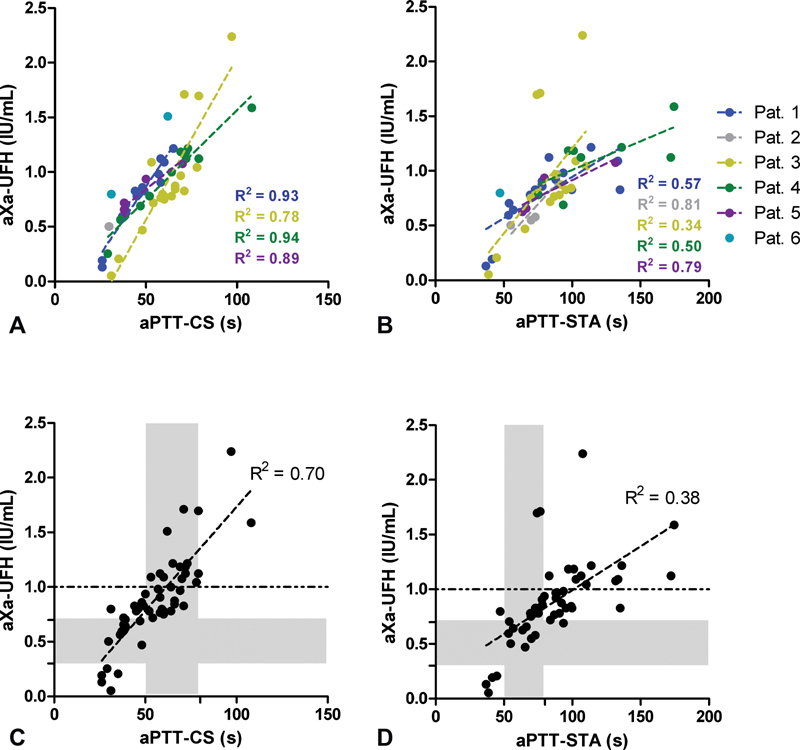
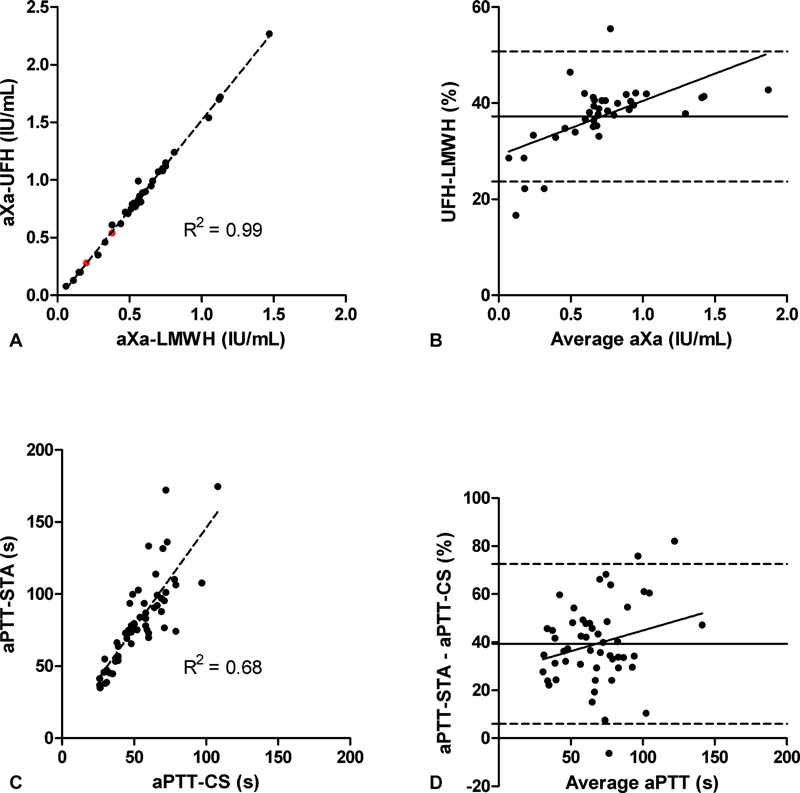
Severe cases of coronavirus disease 2019 (COVID-19) can require continuous renal replacement therapy (CRRT) and/or extracorporeal membrane oxygenation (ECMO). Unfractionated heparin (UFH) to prevent circuit clotting is mandatory but monitoring is complicated by (pseudo)-heparin resistance. In this observational study, we compared two different activated partial thromboplastin time (aPTT) assays and a chromogenic anti-Xa assay in COVID-19 patients on CRRT or ECMO in relation to their UFH dosages and acute phase reactants. The aPTT (optical [aPTT-CS] and/or mechanical [aPTT-STA] clot detection methods were used), anti-Xa, factor VIII (FVIII), antithrombin III (ATIII), and fibrinogen were measured in 342 samples from 7 COVID-19 patients on CRRT or ECMO during their UFH treatment. Dosage of UFH was primarily based on the aPTT-CS with a heparin therapeutic range (HTR) of 50-80s. Associations between different variables were made using linear regression and Bland-Altman analysis. Dosage of UFH was above 35,000IU/24 hours in all patients. aPTT-CS and aPTT-STA were predominantly within the HTR. Anti-Xa was predominantly above the HTR (0.3-0.7 IU/mL) and ATIII concentration was >70% for all patients; mean FVIII and fibrinogen were 606% and 7.5 g/L, respectively. aPTT-CS correlated with aPTT-STA ( = 0.68) with a bias of 39.3%. Correlation between aPTT and anti-Xa was better for aPTT-CS (0.78 ≤ ≤ 0.94) than for aPTT-STA (0.34 ≤ ≤ 0.81). There was no general correlation between the aPTT-CS and ATIII, FVIII, fibrinogen, thrombocytes, C-reactive protein, or ferritin. All included COVID-19 patients on CRRT or ECMO conformed to the definition of heparin resistance. A patient-specific association was found between aPTT and anti-Xa. This association could not be explained by FVIII or fibrinogen.
2019冠状病毒病(COVID-19)重症病例可能需要持续肾脏替代治疗(CRRT)和/或体外膜肺氧合(ECMO)。必须使用普通肝素(UFH)来防止体外循环凝血,但(假性)肝素抵抗会使监测变得复杂。在这项观察性研究中,我们比较了两种不同的活化部分凝血活酶时间(aPTT)检测方法和一种发色抗Xa检测方法,用于接受CRRT或ECMO治疗的COVID-19患者,涉及他们的UFH剂量和急性期反应物。
在7例接受CRRT或ECMO治疗的COVID-19患者的UFH治疗期间,对342份样本进行了aPTT(采用光学[aPTT-CS]和/或机械[aPTT-STA]凝血检测方法)、抗Xa、因子VIII(FVIII)、抗凝血酶III(ATIII)和纤维蛋白原的检测。UFH剂量主要基于aPTT-CS,肝素治疗范围(HTR)为50-80秒。使用线性回归和Bland-Altman分析对不同变量之间的关联进行分析。
所有患者的UFH剂量均高于35,000IU/24小时。aPTT-CS和aPTT-STA主要处于HTR范围内。抗Xa主要高于HTR(0.3-0.7IU/mL),所有患者的ATIII浓度均>70%;平均FVIII和纤维蛋白原分别为606%和7.5g/L。aPTT-CS与aPTT-STA相关(r=0.68),偏差为39.3%。aPTT-CS的aPTT与抗Xa之间的相关性(0.78≤r≤0.94)优于aPTT-STA(0.34≤r≤0.81)。aPTT-CS与ATIII、FVIII、纤维蛋白原、血小板、C反应蛋白或铁蛋白之间没有普遍相关性。
所有纳入的接受CRRT或ECMO治疗的COVID-19患者均符合肝素抵抗的定义。发现aPTT与抗Xa之间存在患者特异性关联。这种关联无法用FVIII或纤维蛋白原解释。