Division of Nephrology, University Health Network, 200 Elizabeth Street, 8N room 846, Toronto, ON, M5G 2C4, Canada.
BMC Nephrol. 2020 Nov 25;21(1):508. doi: 10.1186/s12882-020-02159-z.
Increased right ventricular systolic pressure (RVSP), a surrogate marker for pulmonary hypertension, is common in patients with end-stage kidney disease. Limited data suggest improvement of RVSP with intensive dialysis, but it is unknown whether these improvements translate to better clinical outcomes.
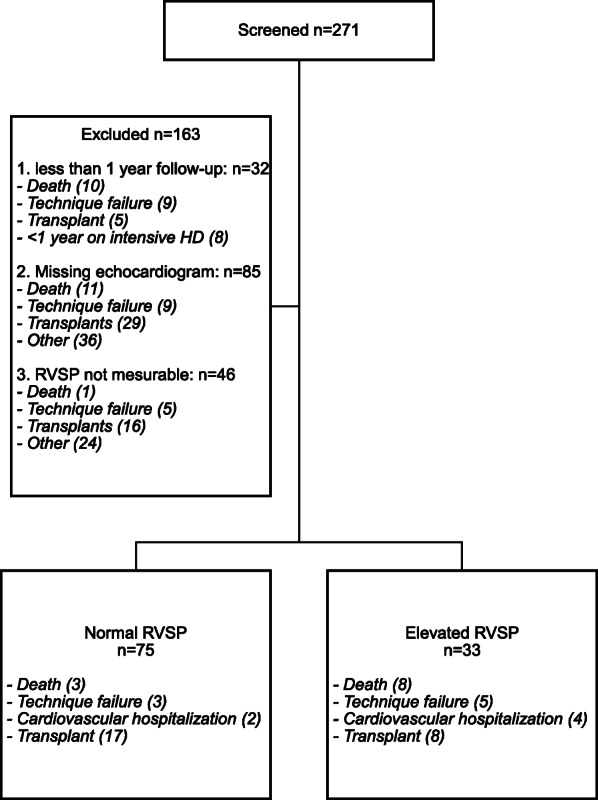
We conducted a retrospective single center cohort study at the Toronto General Hospital. All patients who performed intensive home hemodialysis (IHHD) for at least a year between 1999 and 2017, and who had a baseline as well as a follow-up echocardiogram more than a year after IHHD, were included. Patients were categorized into two groups based on the RVSP at follow-up: elevated (≥ 35 mmHg) and normal RVSP. Multivariate and cox regression analyses were done to identify risk factors for elevated RVSP at follow-up and reaching the composite endpoint (death, cardiovascular hospitalization, treatment failure), respectively.
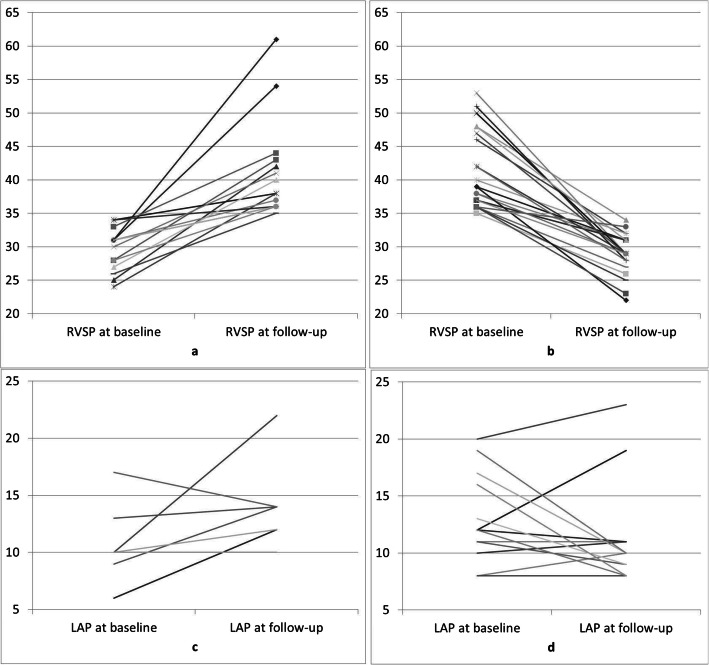
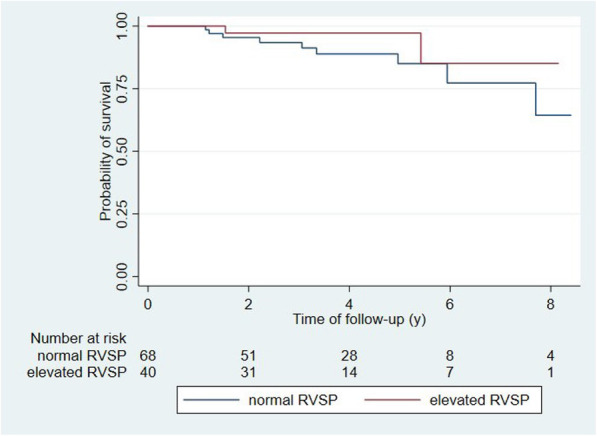
One hundred eight patients were included in the study. At baseline, 63% (68/108) of patients had normal RVSP and 37% (40/108) having elevated RVSP. After a follow-up of 4 years, 70% (76/108) patient had normal RVSP while 30% (32/108) had elevated RVSP. 8 (10%) out of the 76 patients with normal RVSP and 15 (47%) out of the 32 patients with elevated RVSP reached the composite endpoint of death, cardiovascular hospitalization or technique failure. In a multivariate analysis, age, diabetes and smoking were not associated with elevated RVSP at follow-up. Elevated RVSP at baseline was not associated with a higher likelihood in reaching the composite endpoint or mortality.
Mean RVSP did not increase in patients on IHHD over time, and maintenance of normal RVSP was associated with better clinical outcomes.
右心室收缩压(RVSP)升高是肺动脉高压的替代标志物,在终末期肾病患者中很常见。有限的数据表明强化透析可改善 RVSP,但尚不清楚这些改善是否转化为更好的临床结局。
我们在多伦多总医院进行了一项回顾性单中心队列研究。纳入了 1999 年至 2017 年间至少进行了一年家庭强化血液透析(IHHD)且 IHHD 后一年以上有基线和随访超声心动图的所有患者。根据随访时的 RVSP 将患者分为两组:RVSP 升高(≥35mmHg)和 RVSP 正常。进行了多变量和 Cox 回归分析,以确定随访时 RVSP 升高和达到复合终点(死亡、心血管住院、治疗失败)的危险因素。
本研究纳入了 108 例患者。基线时,63%(68/108)的患者 RVSP 正常,37%(40/108)的患者 RVSP 升高。随访 4 年后,70%(76/108)的患者 RVSP 正常,30%(32/108)的患者 RVSP 升高。在 76 例 RVSP 正常的患者中,有 8 例(10%)达到了死亡、心血管住院或技术失败的复合终点,而在 32 例 RVSP 升高的患者中,有 15 例(47%)达到了该复合终点。多变量分析显示,年龄、糖尿病和吸烟与随访时 RVSP 升高无关。基线时 RVSP 升高与更高的复合终点发生率或死亡率无关。
IHHD 患者的 RVSP 均值随时间推移并未增加,而 RVSP 正常与更好的临床结局相关。