MRN Medical Research Network GmbH, Postgasse 11/22, A-1010, Vienna, Austria.
Center for Pharmacology and Analysis (CEPHA) s.r.o, Plzeň, Czech Republic.
BMC Pharmacol Toxicol. 2020 Nov 25;21(1):82. doi: 10.1186/s40360-020-00462-x.
To study the pharmacokinetic and -dynamic behavior of landiolol in the presence of dobutamine in healthy subjects of European ancestry.
We conducted a single-center, prospective randomized study in 16 healthy subjects each receiving an infusion of dobutamine sufficient to increase heart rate by 30 bpm followed by a 60 min infusion of 10 μg/kg/min landiolol.
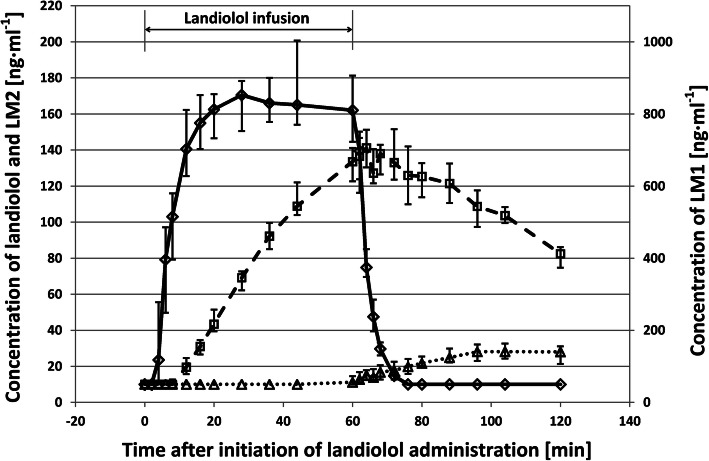
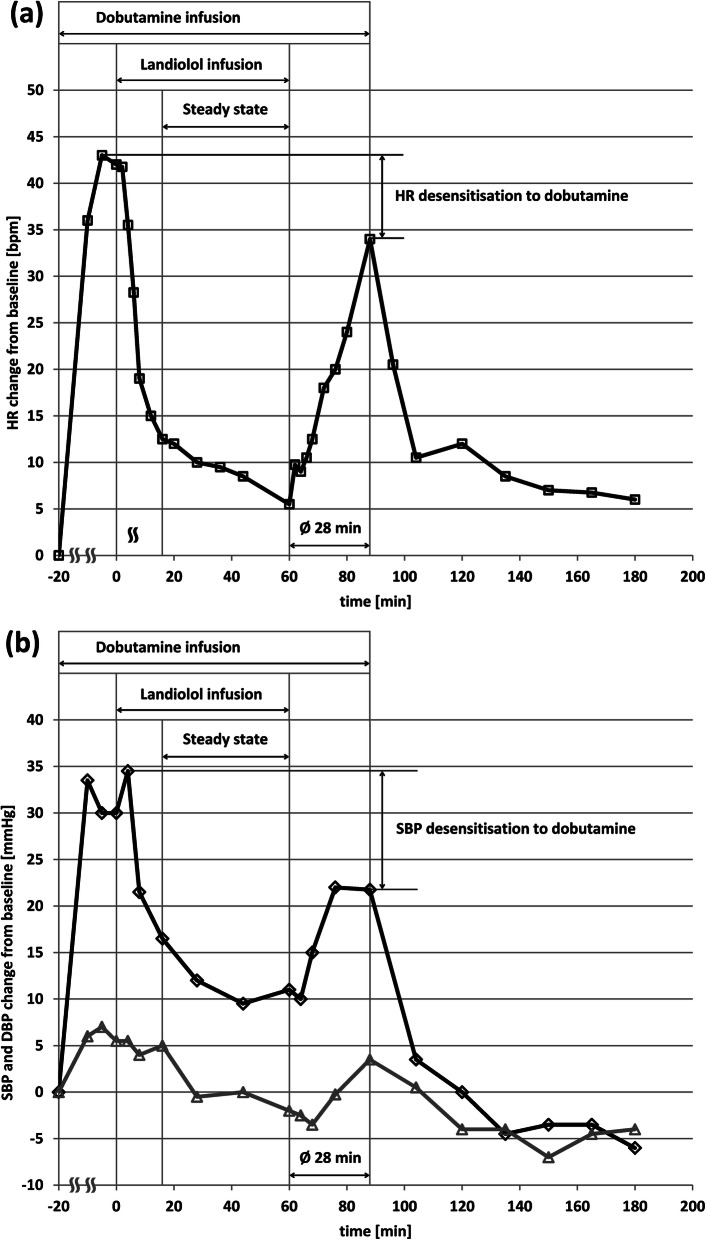
Dobutamine-induced increases in heart rate were stable for at least 20 min before a 60 min landiolol- infusion was started. The dobutamine effects were rapidly antagonized by landiolol within 16 min. A further slight decrease in heart rate during 20-60 min of the landiolol infusion occurred as well. Upon termination of landiolol infusion, heart rate and blood pressure recovered rapidly in response to the persisting dobutamine infusion but did not return to the maximum values before landiolol infusion. The pharmacokinetic parameters of landiolol in presence of dobutamine showed a short half-life (3.5 min) and a low distribution volume (0.3 l/kg). No serious adverse events were observed.
Landiolol can antagonize the dobutamine-induced increases in heart rate and blood pressure in a fast way. A rapid bradycardic effect until steady-state plasma levels is followed by a slow heart rate reduction. The latter can be attributed to an early desensitization to dobutamine. Consequently, after termination of landiolol, the heart rate did not achieve maximum pre-landiolol values. The pharmacokinetics of landiolol during dobutamine infusion are similar when compared to short- and long-term data in Caucasian subjects. Landiolol in the given dose can thus serve as an antagonist of dobutamine-induced cardiac effects.
Registration number 2010-023311-34 at the EU Clinical Trials Register, registration date 2010-12-21.
研究拉替洛尔在欧洲血统健康受试者中与多巴酚丁胺同时存在时的药代动力学和药效动力学行为。
我们进行了一项单中心、前瞻性随机研究,共纳入 16 名健康受试者,每位受试者均接受多巴酚丁胺输注,以增加心率 30bpm,随后给予 60 分钟 10μg/kg/min 拉替洛尔输注。
在开始 60 分钟拉替洛尔输注之前,多巴酚丁胺诱导的心率增加至少稳定 20 分钟。拉替洛尔在 16 分钟内迅速拮抗多巴酚丁胺的作用。在拉替洛尔输注的 20-60 分钟期间,心率也出现进一步轻微下降。当拉替洛尔输注终止时,由于持续输注多巴酚丁胺,心率和血压迅速恢复,但未恢复到拉替洛尔输注前的最大值。存在多巴酚丁胺时拉替洛尔的药代动力学参数显示半衰期短(3.5 分钟),分布容积低(0.3l/kg)。未观察到严重不良事件。
拉替洛尔可以快速拮抗多巴酚丁胺引起的心率和血压升高。在达到稳态血浆水平之前,会出现快速的心动过缓作用,随后心率缓慢下降。后者可归因于对多巴酚丁胺的早期脱敏。因此,拉替洛尔停药后,心率未达到拉替洛尔前的最大值。与白种人群的短期和长期数据相比,拉替洛尔在多巴酚丁胺输注期间的药代动力学相似。在给予的剂量下,拉替洛尔可用作多巴酚丁胺诱导的心脏作用的拮抗剂。
在欧盟临床试验注册中心的注册号为 2010-023311-34,注册日期为 2010 年 12 月 21 日。