Koschut David, Ray Debleena, Li Zhenhua, Giarin Emanuela, Groet Jürgen, Alić Ivan, Kham Shirley Kow-Yin, Chng Wee Joo, Ariffin Hany, Weinstock David M, Yeoh Allen Eng-Juh, Basso Giuseppe, Nižetić Dean
Lee Kong Chian School of Medicine, Nanyang Technological University, Singapore, Singapore.
Department of Paediatrics, Yong Loo Lin School of Medicine, National University of Singapore, Singapore, Singapore.
Oncogene. 2021 Jan;40(4):746-762. doi: 10.1038/s41388-020-01567-7. Epub 2020 Nov 27.
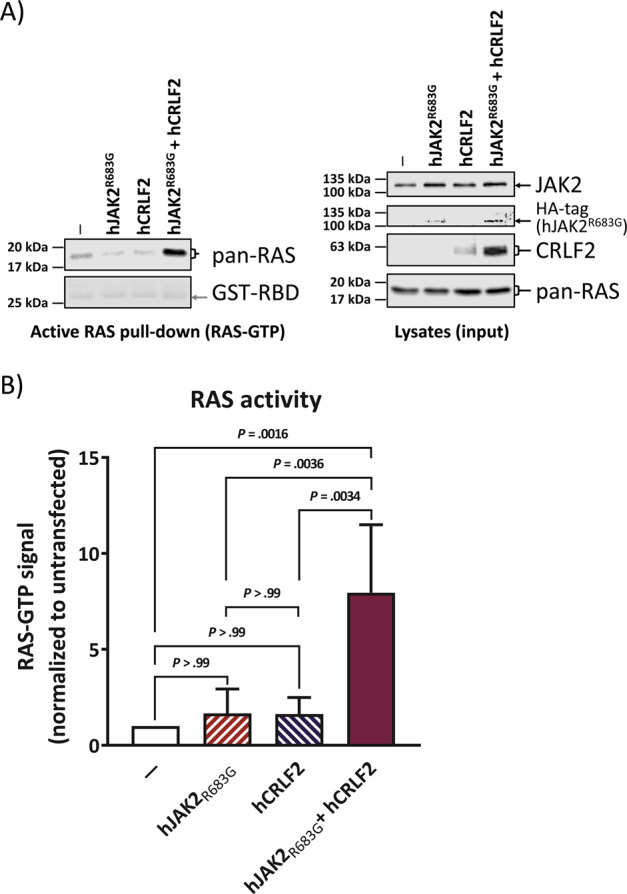
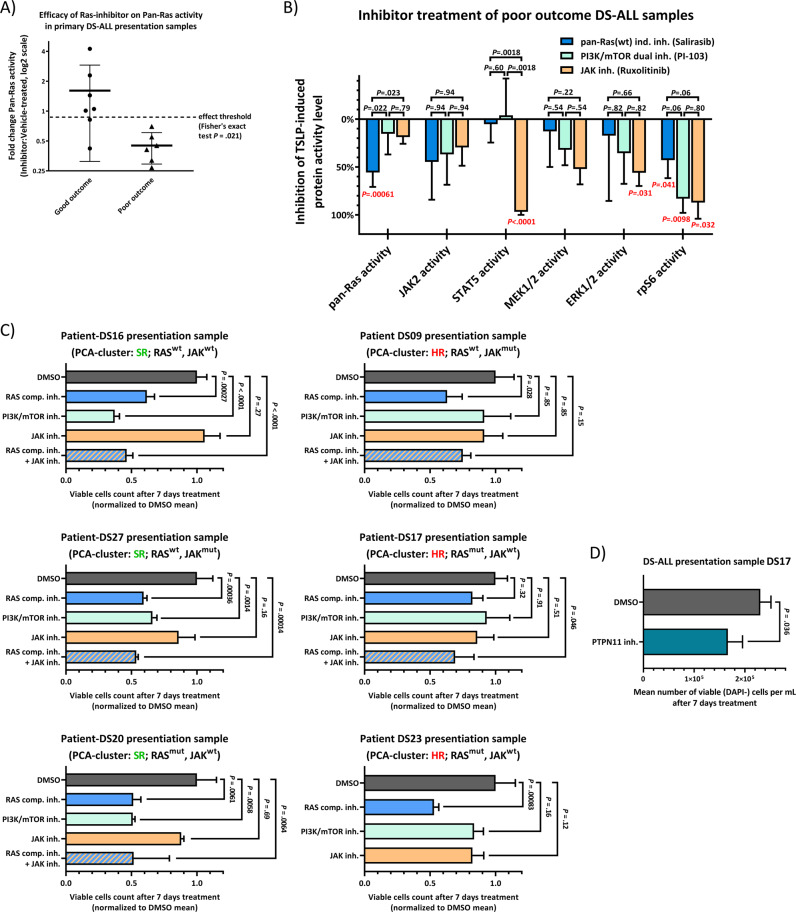
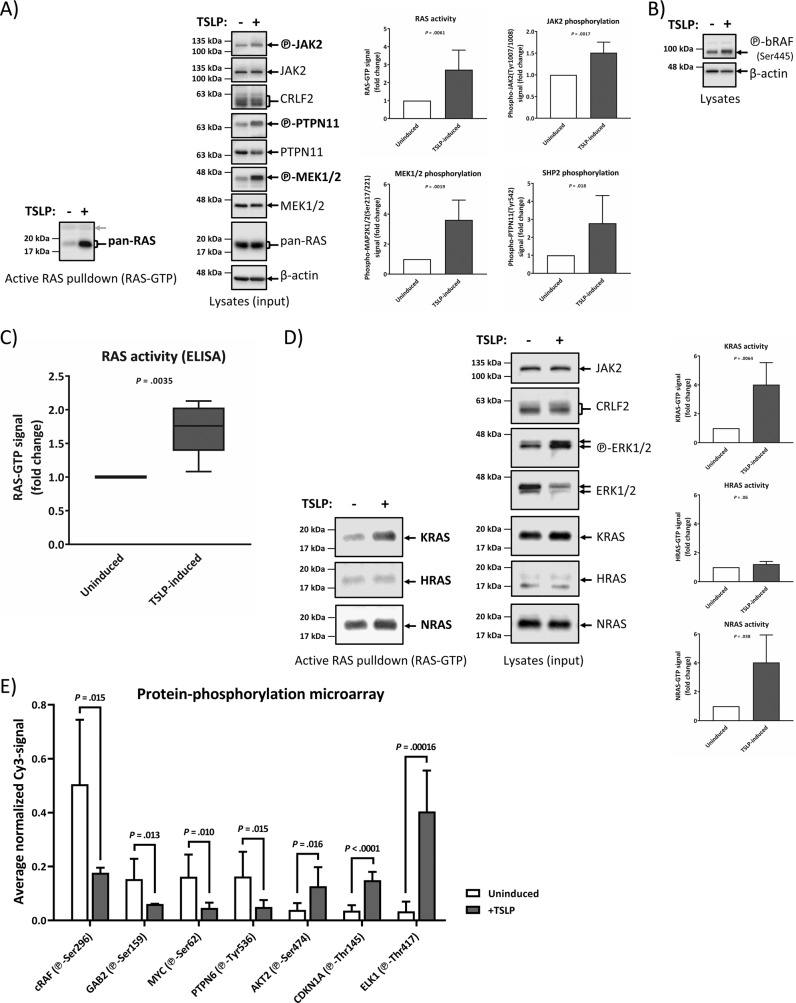
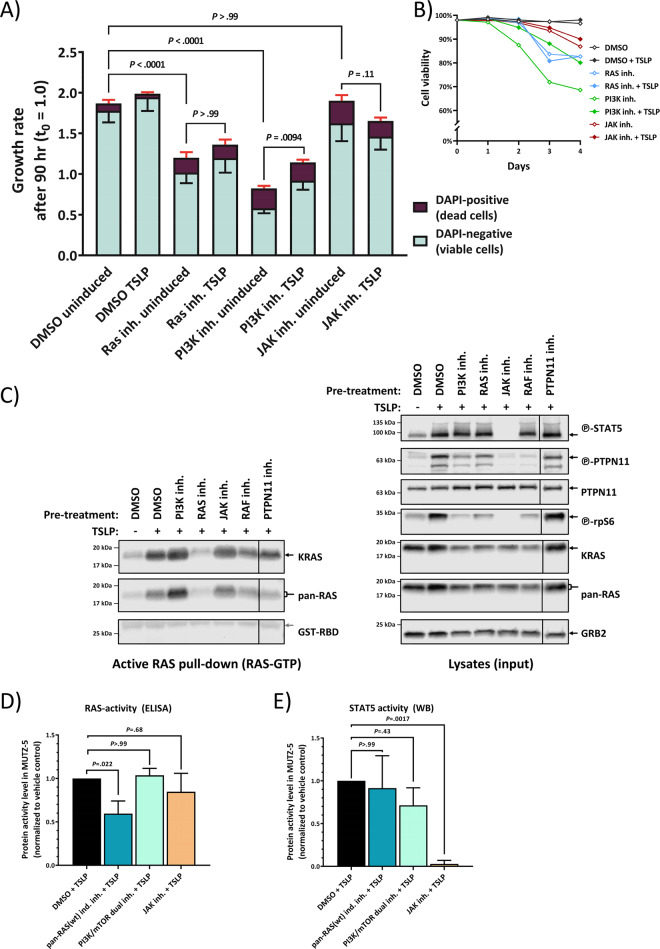
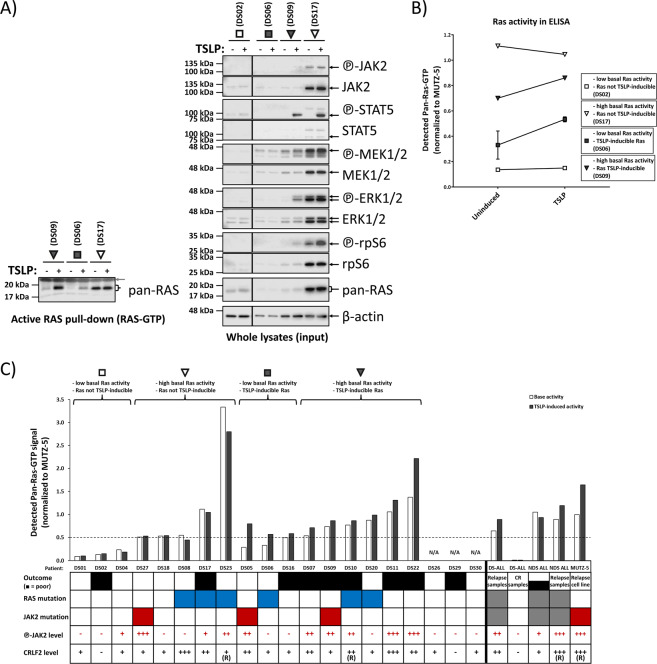
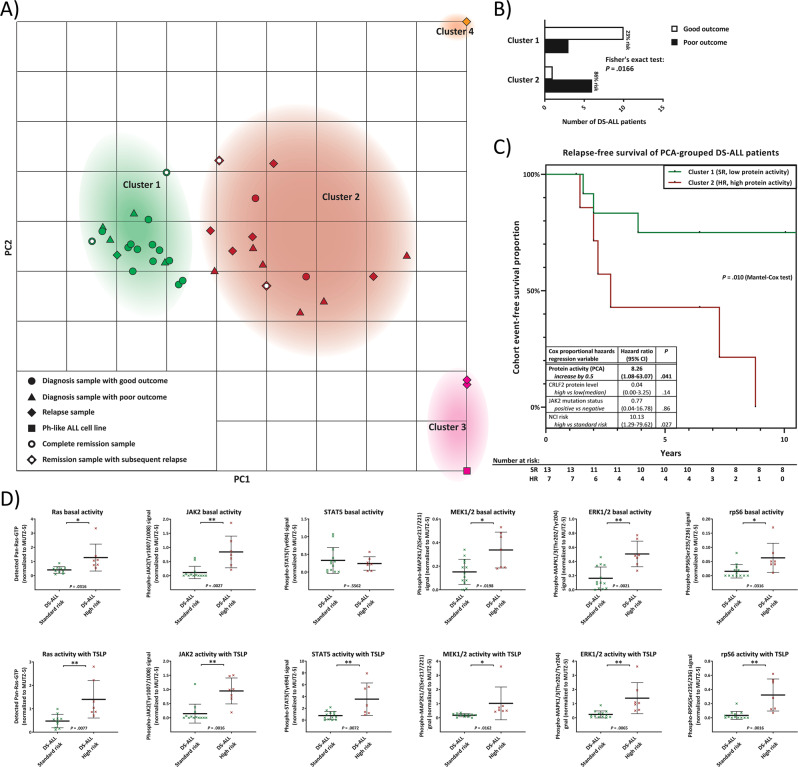
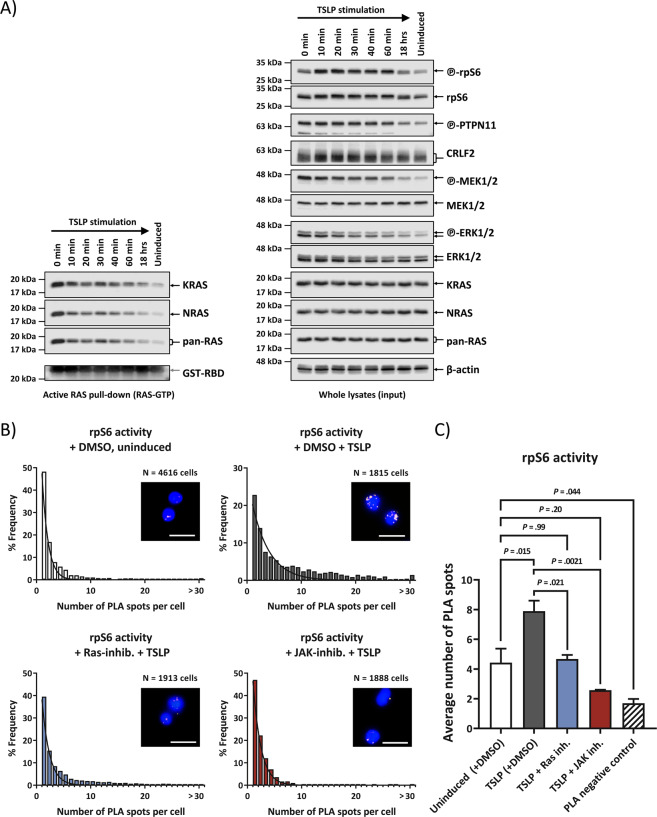
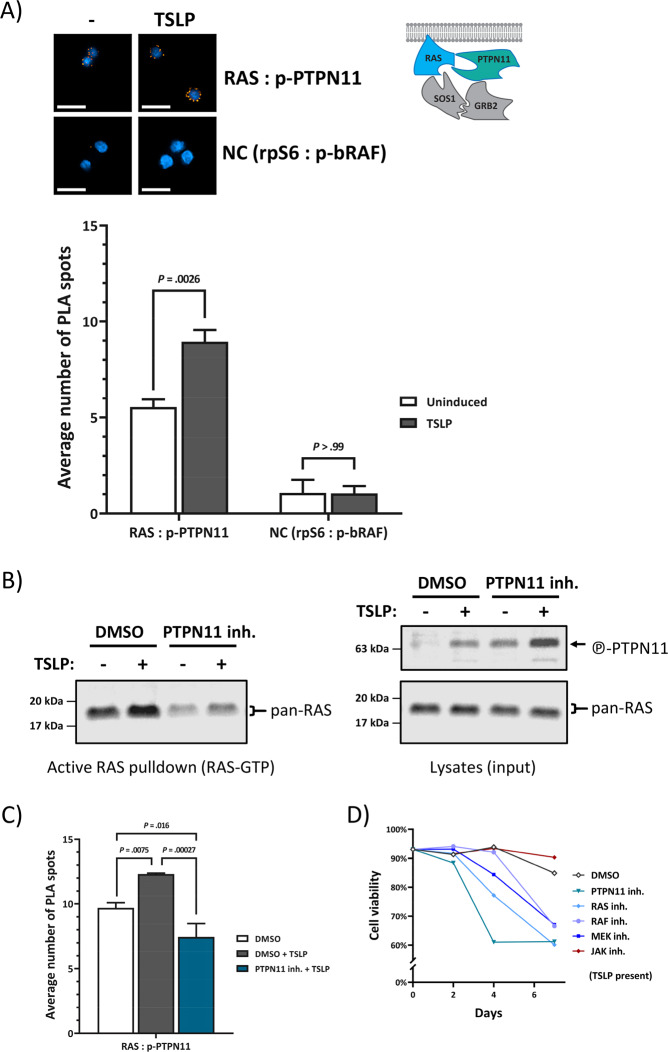
Leukemias are routinely sub-typed for risk/outcome prediction and therapy choice using acquired mutations and chromosomal rearrangements. Down syndrome acute lymphoblastic leukemia (DS-ALL) is characterized by high frequency of CRLF2-rearrangements, JAK2-mutations, or RAS-pathway mutations. Intriguingly, JAK2 and RAS-mutations are mutually exclusive in leukemic sub-clones, causing dichotomy in therapeutic target choices. We prove in a cell model that elevated CRLF2 in combination with constitutionally active JAK2 is sufficient to activate wtRAS. On primary clinical DS-ALL samples, we show that wtRAS-activation is an obligatory consequence of mutated/hyperphosphorylated JAK2. We further prove that CRLF2-ligand TSLP boosts the direct binding of active PTPN11 to wtRAS, providing the molecular mechanism for the wtRAS activation. Pre-inhibition of RAS or PTPN11, but not of PI3K or JAK-signaling, prevented TSLP-induced RAS-GTP boost. Cytotoxicity assays on primary clinical DS-ALL samples demonstrated that, regardless of mutation status, high-risk leukemic cells could only be killed using RAS-inhibitor or PTPN11-inhibitor, but not PI3K/JAK-inhibitors, suggesting a unified treatment target for up to 80% of DS-ALL. Importantly, protein activities-based principal-component-analysis multivariate clusters analyzed for independent outcome prediction using Cox proportional-hazards model showed that protein-activity (but not mutation-status) was independently predictive of outcome, demanding a paradigm-shift in patient-stratification strategy for precision therapy in high-risk ALL.
白血病通常根据获得性突变和染色体重排进行亚型分类,以预测风险/预后并选择治疗方案。唐氏综合征急性淋巴细胞白血病(DS-ALL)的特征是CRLF2重排、JAK2突变或RAS通路突变的频率较高。有趣的是,JAK2和RAS突变在白血病亚克隆中相互排斥,导致治疗靶点选择出现二分法。我们在细胞模型中证明,CRLF2升高与组成性激活的JAK2相结合足以激活野生型RAS。在原发性临床DS-ALL样本中,我们表明野生型RAS激活是JAK2突变/过度磷酸化的必然结果。我们进一步证明,CRLF2配体TSLP增强了活性PTPN11与野生型RAS的直接结合,为野生型RAS激活提供了分子机制。RAS或PTPN11的预抑制,但不是PI3K或JAK信号的预抑制,可阻止TSLP诱导的RAS-GTP增强。对原发性临床DS-ALL样本的细胞毒性试验表明,无论突变状态如何,高危白血病细胞只能用RAS抑制剂或PTPN11抑制剂杀死,而不能用PI3K/JAK抑制剂杀死,这表明高达80%的DS-ALL有统一的治疗靶点。重要的是,使用Cox比例风险模型对基于蛋白质活性的主成分分析多变量聚类进行独立预后预测分析表明,蛋白质活性(而非突变状态)可独立预测预后,这要求在高危ALL的精准治疗患者分层策略上进行范式转变。