Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, George Washington University, Washington, DC.
Division of Pathology and Laboratory Medicine, Children's National Hospital, Washington, DC.
Am J Obstet Gynecol. 2021 Jul;225(1):85.e1-85.e11. doi: 10.1016/j.ajog.2020.11.035. Epub 2020 Nov 26.
Every 2 minutes, there is a pregnancy-related death worldwide, with one-third caused by severe postpartum hemorrhage. Although international trials demonstrated the efficacy of 1000 mg tranexamic acid in treating postpartum hemorrhage, to the best of our knowledge, there are no dose-finding studies of tranexamic acid on pregnant women for postpartum hemorrhage prevention.
This study aimed to determine the optimal tranexamic acid dose needed to prevent postpartum hemorrhage.
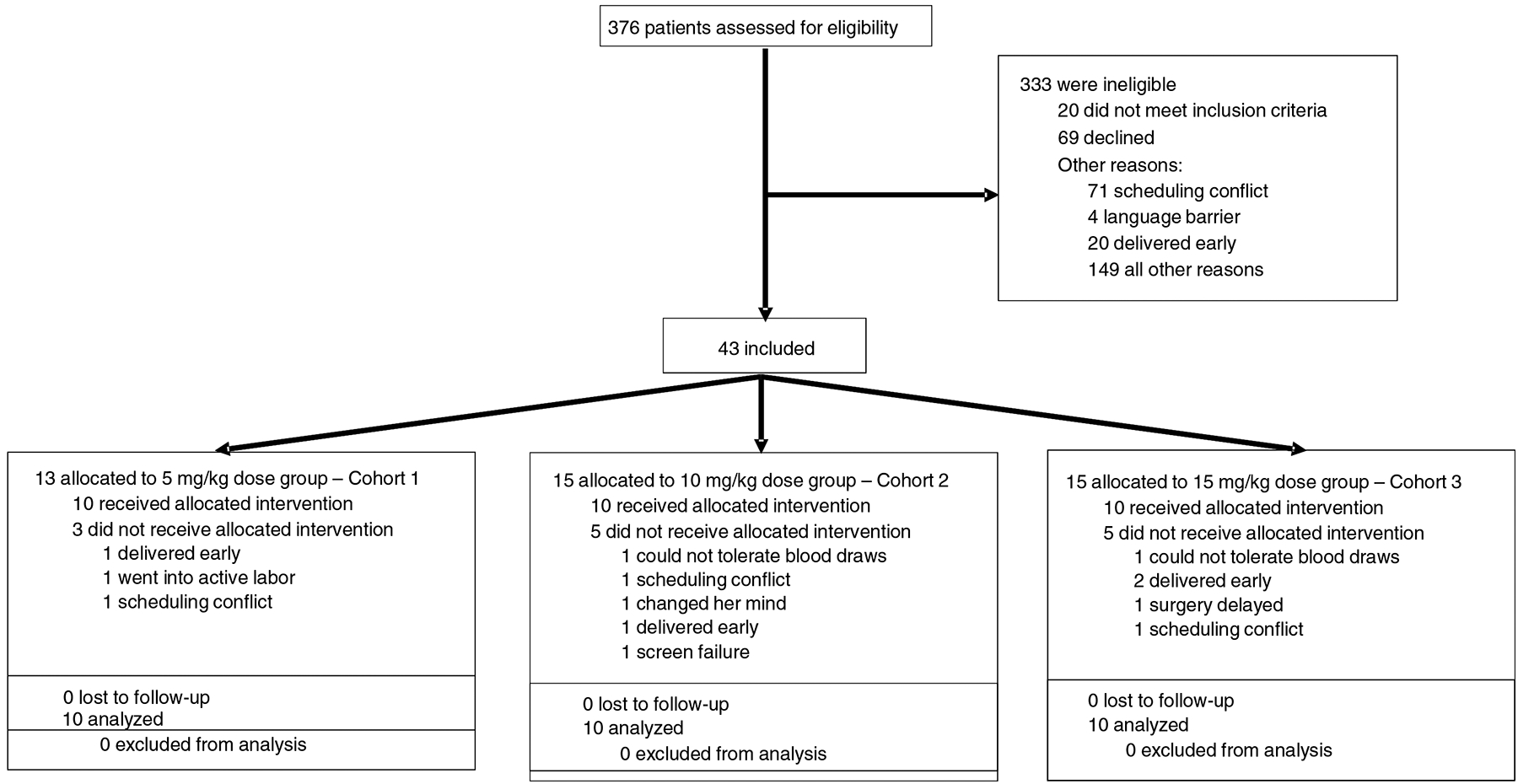
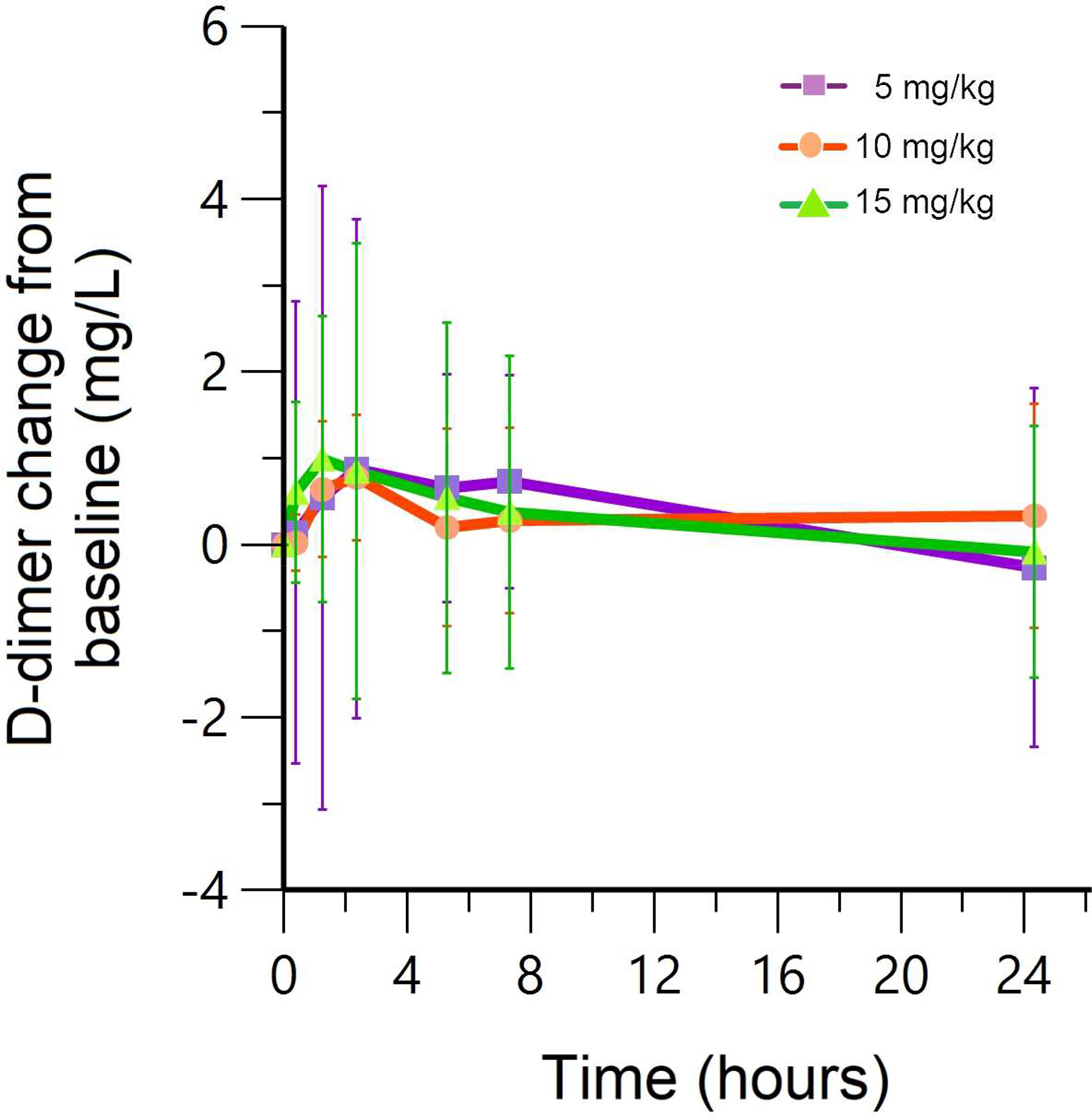
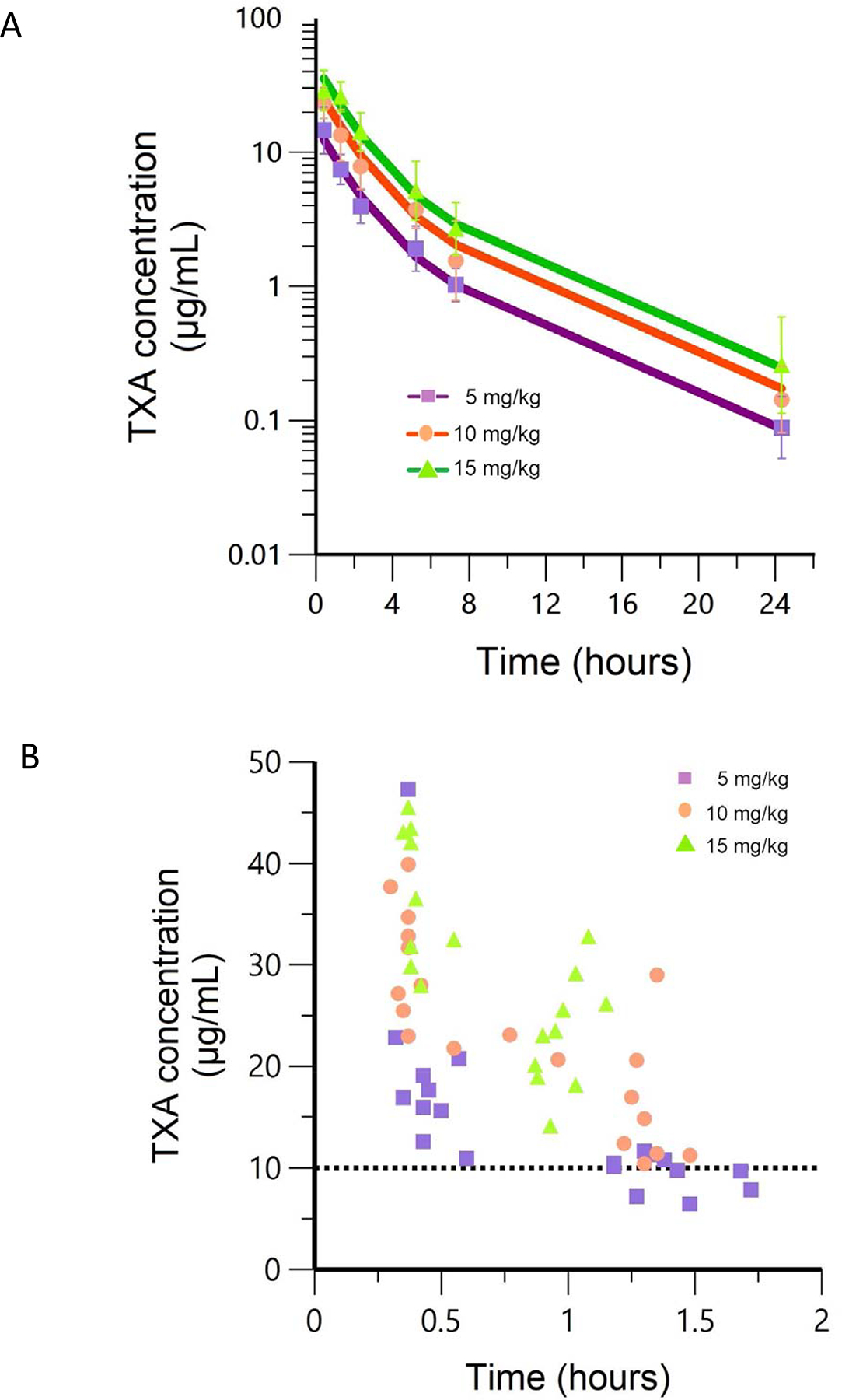
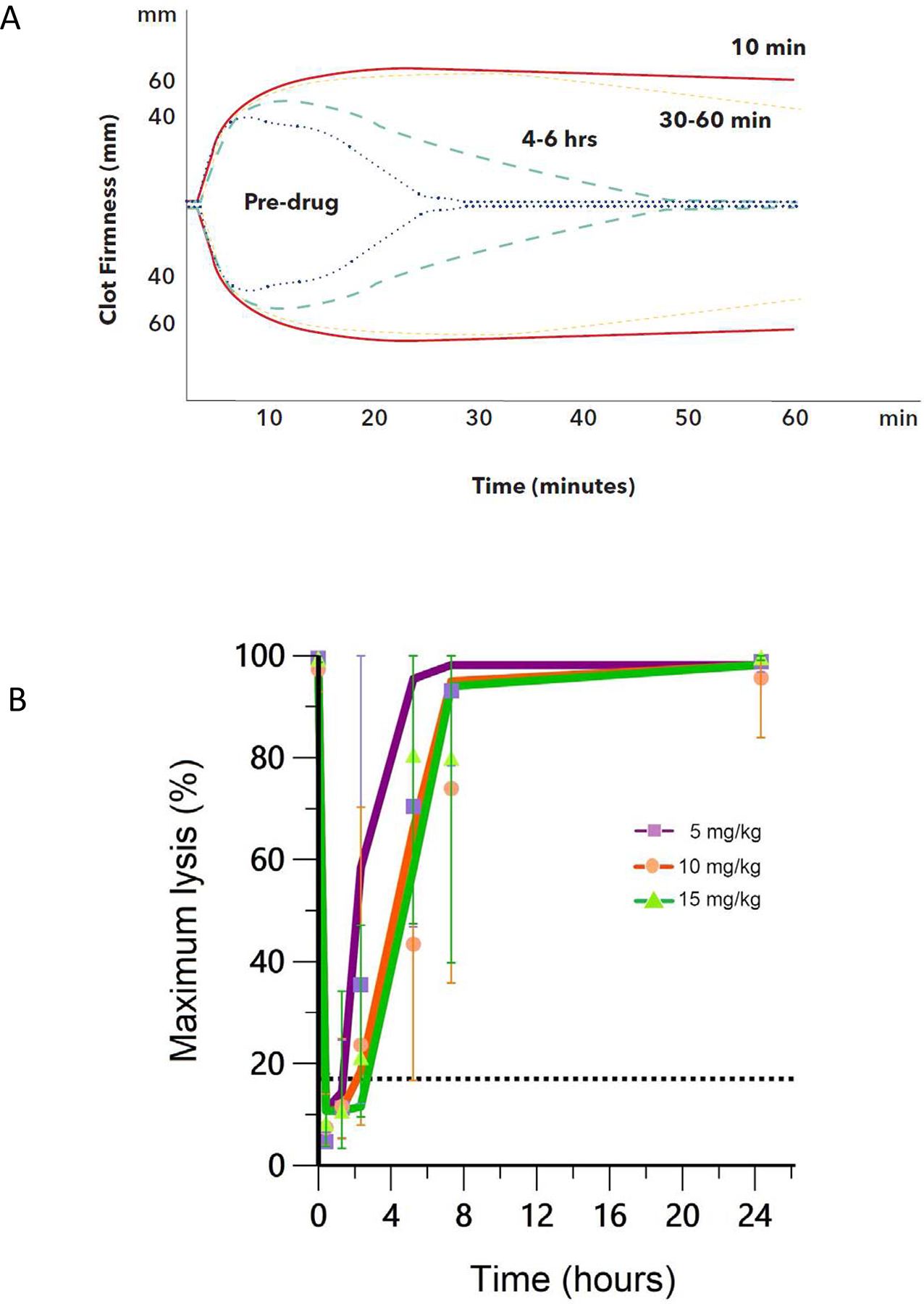
We enrolled 30 pregnant women undergoing scheduled cesarean delivery in an open-label, dose ranging study. Subjects were divided into 3 cohorts receiving 5, 10, or 15 mg/kg (maximum, 1000 mg) of intravenous tranexamic acid at umbilical cord clamping. The inclusion criteria were ≥34 week's gestation and normal renal function. The primary endpoints were pharmacokinetic and pharmacodynamic profiles. Tranexamic acid plasma concentration of >10 μg/mL and maximum lysis of <17% were defined as therapeutic targets independent to the current study. Rotational thromboelastometry of tissue plasminogen activator-spiked samples was used to evaluate pharmacodynamic profiles at time points up to 24 hours after tranexamic acid administration. Safety was assessed by plasma thrombin generation, D-dimer, and tranexamic acid concentrations in breast milk.
There were no serious adverse events including venous thromboembolism. Plasma concentrations of tranexamic acid increased in a dose-proportional manner. The lowest dose cohort received an average of 448±87 mg tranexamic acid. Plasma tranexamic acid exceeded 10 μg/mL and maximum lysis was <17% at >1 hour after administration for all tranexamic acid doses tested. Median estimated blood loss for cohorts receiving 5, 10, or 15 mg/kg tranexamic acid was 750, 750, and 700 mL, respectively. Plasma thrombin generation did not increase with higher tranexamic acid concentrations. D-dimer changes from baseline were not different among the cohorts. Breast milk tranexamic acid concentrations were 1% or less than maternal plasma concentrations.
Although large randomized trials are necessary to support the clinical efficacy of tranexamic acid for prophylaxis, we propose an optimal dose of 600 mg in future tranexamic acid efficacy studies to prevent postpartum hemorrhage.
全球每两分钟就有一名与妊娠相关的产妇死亡,其中三分之一是由产后大出血引起的。尽管国际试验已经证明了 1000 毫克氨甲环酸治疗产后出血的疗效,但就我们所知,目前还没有关于氨甲环酸预防产后出血的剂量探索研究。
本研究旨在确定预防产后出血所需的氨甲环酸最佳剂量。
我们进行了一项开放标签、剂量范围研究,共纳入 30 名计划行剖宫产的孕妇。受试者被分为 3 组,在脐带夹闭时分别接受 5、10 或 15mg/kg(最大剂量 1000mg)的静脉氨甲环酸。纳入标准为妊娠 34 周及以上且肾功能正常。主要终点是药代动力学和药效学特征。本研究将氨甲环酸血浆浓度>10μg/mL 和最大溶解率<17%定义为与当前研究无关的治疗目标。在氨甲环酸给药后长达 24 小时的时间点,使用组织纤溶酶原激活物加样的旋转血栓弹性描记术评估药效学特征。通过血浆凝血酶生成、D-二聚体和氨甲环酸在母乳中的浓度评估安全性。
无严重不良事件,包括静脉血栓栓塞。氨甲环酸的血浆浓度呈剂量依赖性增加。最低剂量组平均接受 448±87mg 氨甲环酸。所有测试的氨甲环酸剂量组在给药后 1 小时以上,氨甲环酸血浆浓度均超过 10μg/mL,最大溶解率<17%。接受 5、10 或 15mg/kg 氨甲环酸的组,中位估计失血量分别为 750、750 和 700mL。随着氨甲环酸浓度的增加,血浆凝血酶生成没有增加。各队列的 D-二聚体变化与基线相比无差异。母乳中的氨甲环酸浓度为 1%或低于母体血浆浓度。
尽管需要进行大型随机试验来支持氨甲环酸在预防方面的临床疗效,但我们建议在未来的氨甲环酸疗效研究中采用 600mg 的最佳剂量来预防产后出血。