Department of Microbiology, Monash Health, Clayton, Victoria, Australia.
Department of Infectious Diseases, Monash Health, Clayton, Victoria, Australia.
Ann Clin Microbiol Antimicrob. 2020 Nov 30;19(1):57. doi: 10.1186/s12941-020-00400-z.
Cefiderocol, ceftazidime-avibactam, ceftolozane-tazobactam, intravenous fosfomycin and plazomicin represent potential carbapenem sparing agents for extended-spectrum-beta-lactamase or AmpC beta-lactamase producing Escherichia coli infection. However, available data is limited in predicting the volume of carbapenem therapy which could be substituted and real-world contraindications.
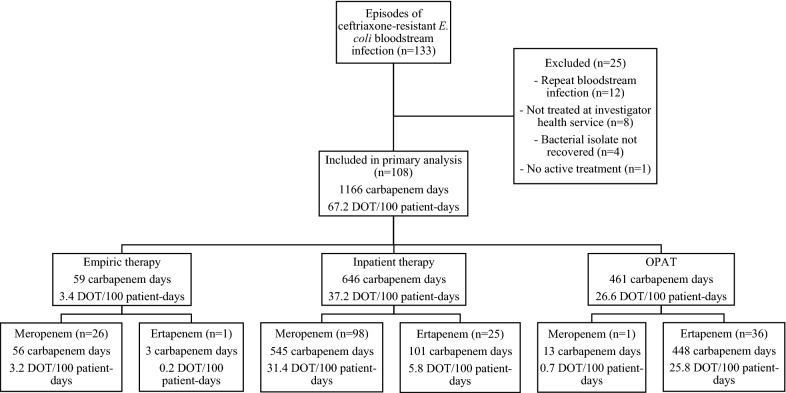
We determined the number of carbapenem days of therapy (DOT) which could be substituted and frequent contraindications accounting for antimicrobial susceptibility and site of infection in an unselected cohort with ceftriaxone-non-susceptible E. coli bacteremia at a single health network from 2015 to 2016. Individual patient data was used to calculate DOT and substitution for each agent.
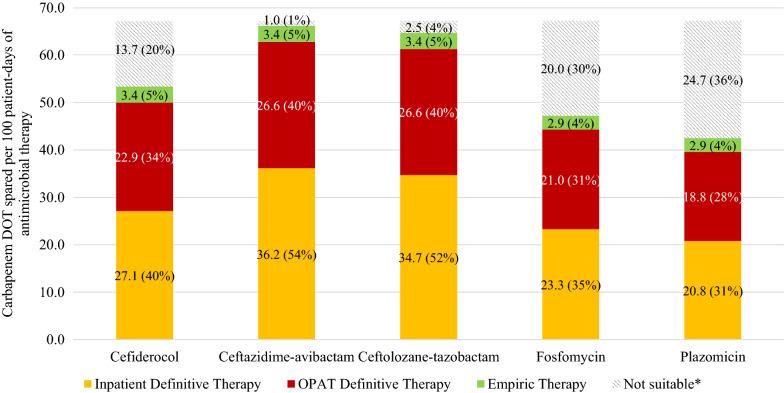
There were 108 episodes of E. coli bacteremia resulting in 67.2 carbapenem DOT/100 patient-days of antimicrobial therapy administered. Ceftazidime-avibactam could be used to substitute 36.2 DOT/100 patient-days (54%) for inpatient definitive therapy, ceftolozane-tazobactam for 34.7 DOT/100 patient-days (52%), cefiderocol for 27.1 DOT/100 patient-days (40%), fosfomycin for 23.3 DOT /100 patient-days (35%) and plazomicin for 27.1 DOT/100 patient-days (40%). Non-urinary tract source of infection was the most frequent contraindication to fosfomycin (25), plazomicin (26) and cefiderocol (26). Use in outpatient parenteral antimicrobial therapy (OPAT) programs accounted for 40% of DOT, all of which could be substituted if stability data allowed for ceftazidime-avibactam and ceftolozane-tazobactam.
All tested agents could be used to replace a significant volume of carbapenem therapy. Establishing stability of these agents for use in OPAT is required for maximizing their use as carbapenem sparing agents while randomized clinical data is awaited for some of these agents in resistant E. coli bacteremia.
头孢地尔、头孢他啶-阿维巴坦、头孢洛扎-他唑巴坦、静脉注射磷霉素和硫酸帕米霉素是产超广谱β-内酰胺酶或 AmpCβ-内酰胺酶的大肠埃希菌感染的潜在碳青霉烯类药物节约剂。然而,可用数据在预测可替代的碳青霉烯类药物治疗量和实际的禁忌症方面存在局限性。
我们确定了在 2015 年至 2016 年期间,在一个单一的健康网络中,对头孢曲松耐药的大肠埃希菌菌血症患者进行了一项无选择队列研究,该研究使用抗菌药物治疗的每 100 名患者-天中碳青霉烯类药物治疗天数(DOT)的替代和常见禁忌症,以评估抗菌药物敏感性和感染部位。使用个体患者数据计算每种药物的 DOT 和替代量。
共有 108 例大肠埃希菌菌血症,导致 67.2 碳青霉烯类药物 DOT/100 患者-天的抗菌药物治疗。头孢他啶-阿维巴坦可用于替代 36.2 天 DOT/100 患者-天(54%)的住院治疗,头孢洛扎-他唑巴坦为 34.7 天 DOT/100 患者-天(52%),头孢地尔为 27.1 天 DOT/100 患者-天(40%),磷霉素为 23.3 天 DOT/100 患者-天(35%),硫酸帕米霉素为 27.1 天 DOT/100 患者-天(40%)。非尿路来源的感染是磷霉素(25%)、硫酸帕米霉素(26%)和头孢地尔(26%)最常见的禁忌症。门诊静脉输注抗菌药物治疗(OPAT)方案占 DOT 的 40%,如果稳定性数据允许使用头孢他啶-阿维巴坦和头孢洛扎-他唑巴坦,所有这些都可以替代。
所有测试的药物都可以用来替代大量的碳青霉烯类药物治疗。在等待这些药物在耐药大肠埃希菌菌血症中的随机临床试验数据的同时,需要确定这些药物在 OPAT 中的稳定性,以最大限度地发挥它们作为碳青霉烯类药物节约剂的作用。