School of Biological Science and Medical Engineering, Southeast University, #2 SiPailou, Nanjing, China.
The Cardiovascular Research Foundation, Columbia University, New York, USA.
Biomed Eng Online. 2020 Nov 30;19(1):90. doi: 10.1186/s12938-020-00832-w.
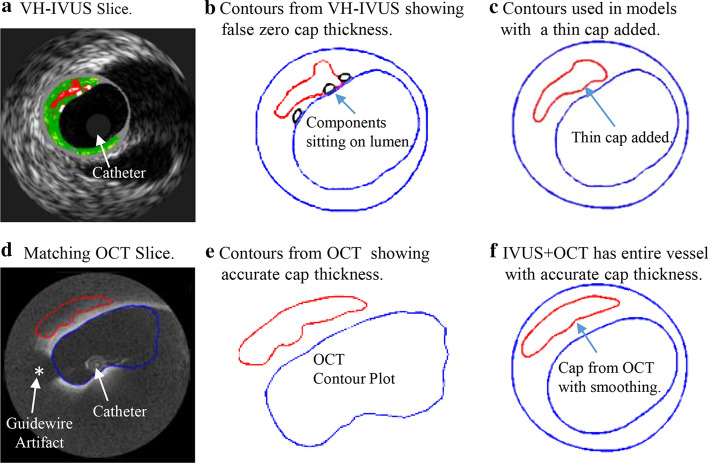
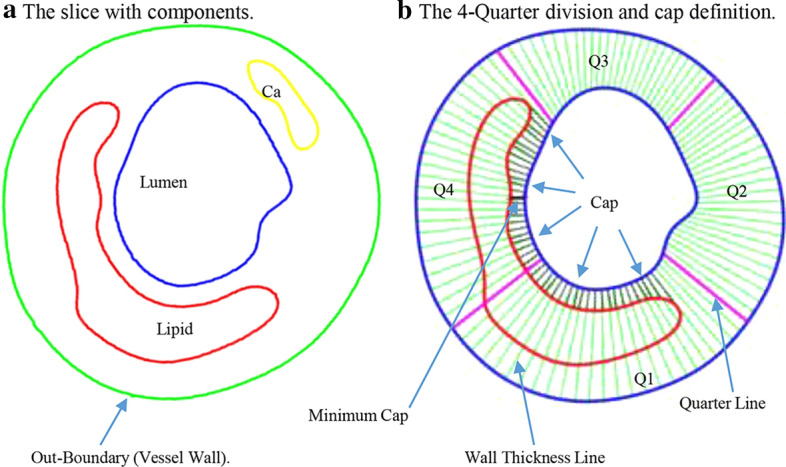
Detecting coronary vulnerable plaques in vivo and assessing their vulnerability have been great challenges for clinicians and the research community. Intravascular ultrasound (IVUS) is commonly used in clinical practice for diagnosis and treatment decisions. However, due to IVUS limited resolution (about 150-200 µm), it is not sufficient to detect vulnerable plaques with a threshold cap thickness of 65 µm. Optical Coherence Tomography (OCT) has a resolution of 15-20 µm and can measure fibrous cap thickness more accurately. The aim of this study was to use OCT as the benchmark to obtain patient-specific coronary plaque cap thickness and evaluate the differences between OCT and IVUS fibrous cap quantifications. A cap index with integer values 0-4 was also introduced as a quantitative measure of plaque vulnerability to study plaque vulnerability.
Data from 10 patients (mean age: 70.4; m: 6; f: 4) with coronary heart disease who underwent IVUS, OCT, and angiography were collected at Cardiovascular Research Foundation (CRF) using approved protocol with informed consent obtained. 348 slices with lipid core and fibrous caps were selected for study. Convolutional Neural Network (CNN)-based and expert-based data segmentation were performed using established methods previously published. Cap thickness data were extracted to quantify differences between IVUS and OCT measurements.
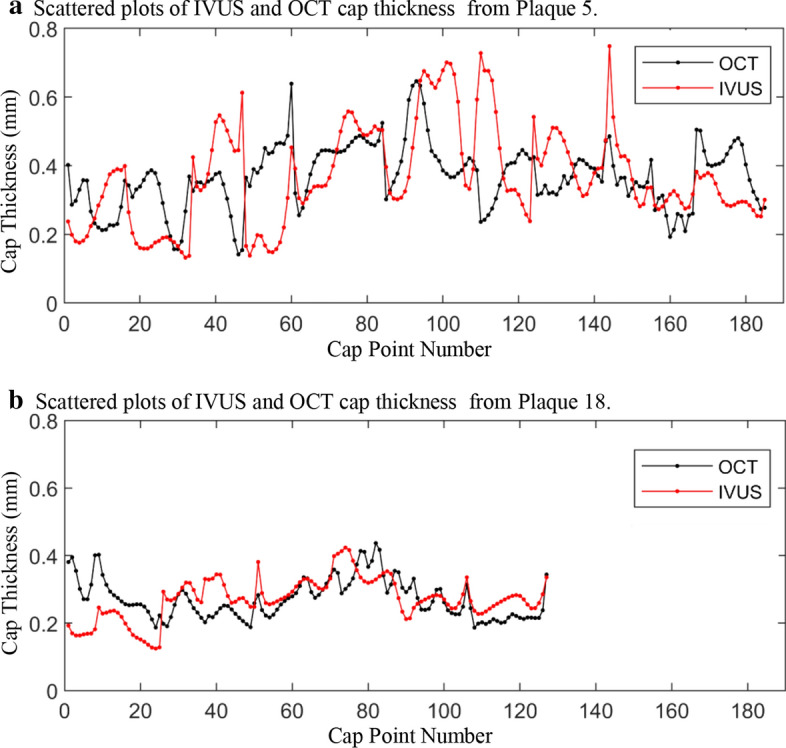
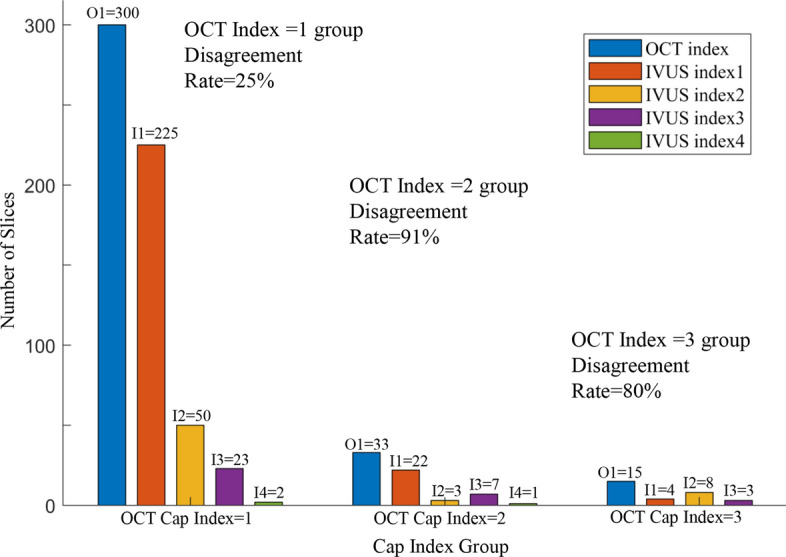
For the 348 slices analyzed, the mean value difference between OCT and IVUS cap thickness measurements was 1.83% (p = 0.031). However, mean value of point-to-point differences was 35.76%. Comparing minimum cap thickness for each plaque, the mean value of the 20 plaque IVUS-OCT differences was 44.46%, ranging from 2.36% to 91.15%. For cap index values assigned to the 348 slices, the disagreement between OCT and IVUS assignments was 25%. However, for the OCT cap index = 2 and 3 groups, the disagreement rates were 91% and 80%, respectively. Furthermore, the observation of cap index changes from baseline to follow-up indicated that IVUS results differed from OCT by 80%.
These preliminary results demonstrated that there were significant differences between IVUS and OCT plaque cap thickness measurements. Large-scale patient studies are needed to confirm our findings.
在体内检测易损斑块并评估其易损性一直是临床医生和研究界的巨大挑战。血管内超声(IVUS)在临床实践中常用于诊断和治疗决策。然而,由于 IVUS 的分辨率有限(约 150-200 µm),不足以检测到阈值帽厚度为 65 µm 的易损斑块。光学相干断层扫描(OCT)的分辨率为 15-20 µm,能够更准确地测量纤维帽厚度。本研究旨在使用 OCT 作为基准来获得患者特定的冠状动脉斑块帽厚度,并评估 OCT 和 IVUS 纤维帽定量之间的差异。还引入了一个整数为 0-4 的帽指数作为斑块易损性的定量指标,以研究斑块易损性。
在心血管研究基金会(CRF),根据获得知情同意的批准方案,收集了 10 名患有冠心病的患者(平均年龄:70.4 岁;男性:6 名;女性:4 名)的 IVUS、OCT 和血管造影数据。选择了 348 个具有脂质核心和纤维帽的切片进行研究。使用先前发表的既定方法进行基于卷积神经网络(CNN)和专家的数据分割。提取帽厚度数据以量化 IVUS 和 OCT 测量值之间的差异。
在分析的 348 个切片中,OCT 和 IVUS 帽厚度测量值之间的平均值差异为 1.83%(p=0.031)。然而,点到点差异的平均值为 35.76%。比较每个斑块的最小帽厚度,20 个斑块 IVUS-OCT 差异的平均值为 44.46%,范围为 2.36%至 91.15%。对于分配给 348 个切片的帽指数值,OCT 和 IVUS 分配之间的不一致率为 25%。然而,对于 OCT 帽指数=2 和 3 组,不一致率分别为 91%和 80%。此外,观察从基线到随访的帽指数变化表明,IVUS 结果与 OCT 相差 80%。
这些初步结果表明,IVUS 和 OCT 斑块帽厚度测量值之间存在显著差异。需要进行大规模的患者研究来证实我们的发现。