Joharatnam-Hogan Nalinie, Wilson William, Shiu Kai Keen, Fusai Giuseppe Kito, Davidson Brian, Hochhauser Daniel, Bridgewater John, Khan Khurum
Department of Gastrointestinal Oncology, University College London Hospital NHS Foundation Trust, London NW1 2PG, UK.
Department of Statistics, Cancer Research UK and UCL Cancer Trials Centre, London W1T 4TJ, UK.
Cancers (Basel). 2020 Nov 27;12(12):3545. doi: 10.3390/cancers12123545.
Despite notable advances in the management of metastatic colorectal cancer (mCRC) over the last two decades, treatment intent in the vast majority of patients remains palliative due to technically unresectable disease, extensive disease, or co-morbidities precluding major surgery. Up to 30% of individuals with mCRC are considered potentially suitable for primary or metastasis-directed multimodal therapy, including surgical resection, ablative techniques, or stereotactic radiotherapy (RT), with the aim of improving survival outcomes. We reviewed the potential benefits of multimodal therapy on the survival of patients with mCRC treated at the UCLH.
Clinical data on baseline characteristics, multimodal treatments, and survival outcomes were retrospectively collected from all patients with mCRC receiving systemic chemotherapy between January 2013 and April 2017. Primary outcome was the impact of multimodal therapy on overall survival, compared to systemic therapy alone, and the effect of different types of multimodal therapy on survival outcome, and was assessed using the Kaplan-Meier approach. All analyses were adjusted for age, gender, and side of primary tumour.
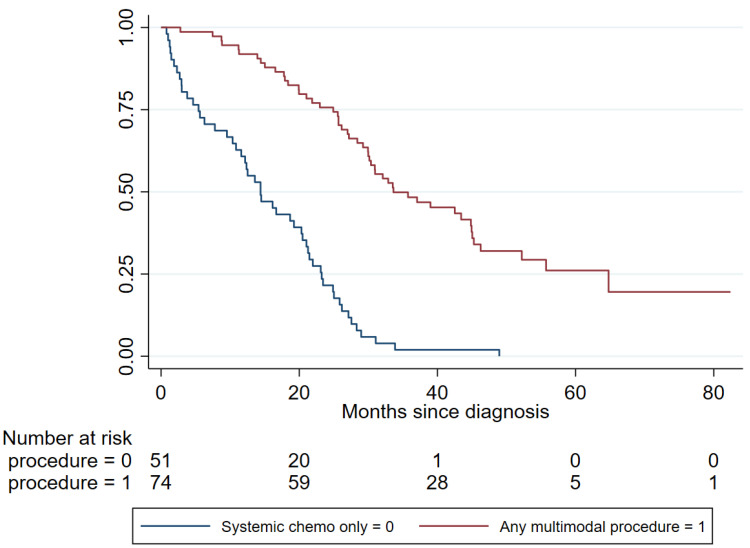
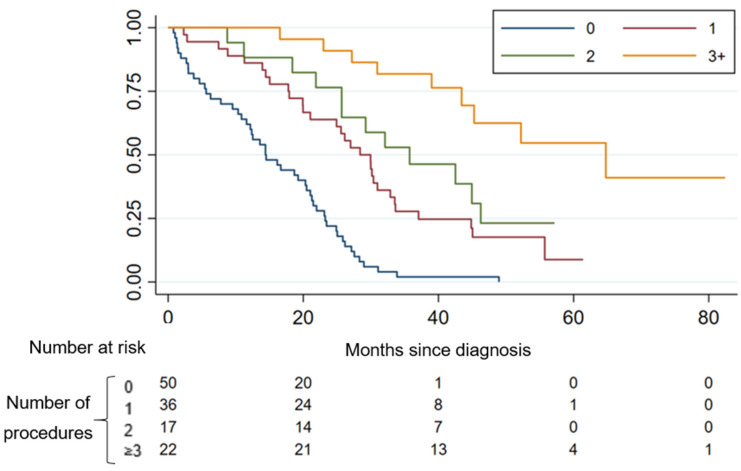
One-hundred and twenty-five patients with mCRC were treated during the study period (median age: 62 years (range 19-89). The liver was the most frequent metastatic site (78%; 97/125). A total of 52% (65/125) had ≥2 lines of systemic chemotherapy. Of the 125 patients having systemic chemotherapy, 74 (59%) underwent multimodal treatment to the primary tumour or metastasis. Median overall survival (OS) was 25.7 months [95% Confidence Interval (CI) 21.5-29.0], and 3-year survival, 26%. Univariate analysis demonstrated that patients who had additional procedures (surgery/ablation/RT) were significantly less likely to die (Hazard Ratio (HR) 0.18, 95% CI 0.12-0.29, < 0.0001) compared to those receiving systemic chemotherapy alone. Increasing number of multimodal procedures was associated with an incremental increase in survival-with median OS 28.4 m, 35.7 m, and 64.8 m, respectively, for 1, 2, or ≥3 procedures (log-rank < 0.0001). After exclusion of those who received systemic chemotherapy only ( = 51), metastatic resections were associated with improved survival (adjusted HR 0.36, 95% CI 0.20-0.63, < 0.0001), confirmed in multivariate analysis. Multiple single-organ procedures did not improve survival.
Multimodal therapy for metastatic bowel cancer is associated with significant survival benefit. Resection/radical RT of the primary and resection of metastatic disease should be considered to improve survival outcomes following multidisciplinary team (MDT) discussion and individual assessment of fitness.
尽管在过去二十年中转移性结直肠癌(mCRC)的治疗取得了显著进展,但由于疾病在技术上无法切除、病变广泛或存在合并症而无法进行大手术,绝大多数患者的治疗目的仍为姑息性治疗。高达30%的mCRC患者被认为可能适合进行原发灶或转移灶导向的多模式治疗,包括手术切除、消融技术或立体定向放射治疗(RT),目的是改善生存结局。我们回顾了多模式治疗对在伦敦大学学院医院(UCLH)接受治疗的mCRC患者生存的潜在益处。
回顾性收集了2013年1月至2017年4月期间所有接受全身化疗的mCRC患者的基线特征、多模式治疗及生存结局的临床数据。主要结局是多模式治疗与单纯全身治疗相比对总生存的影响,以及不同类型多模式治疗对生存结局的影响,并采用Kaplan-Meier方法进行评估。所有分析均对年龄、性别和原发肿瘤部位进行了校正。
在研究期间共治疗了125例mCRC患者(中位年龄:62岁(范围19 - 89岁))。肝脏是最常见的转移部位(78%;97/125)。共有52%(65/125)的患者接受了≥2线的全身化疗。在接受全身化疗的125例患者中,74例(59%)对原发肿瘤或转移灶进行了多模式治疗。中位总生存(OS)为25.7个月[95%置信区间(CI)21.5 - 29.0],3年生存率为26%。单因素分析表明,与仅接受全身化疗的患者相比,接受额外手术(手术/消融/RT)的患者死亡可能性显著降低(风险比(HR)0.18,95% CI 0.12 - 0.29,<0.0001)。多模式手术数量增加与生存率逐步提高相关 - 1次、2次或≥3次手术的中位OS分别为28.4个月、35.7个月和64.8个月(对数秩检验<0.0001)。排除仅接受全身化疗的患者(n = 51)后,转移灶切除与生存改善相关(校正HR 0.36,95% CI 0.20 - 0.63,<0.0001),多因素分析证实了这一点。多次单器官手术并未改善生存。
转移性肠癌的多模式治疗与显著的生存获益相关。在多学科团队(MDT)讨论并对患者身体状况进行个体评估后,应考虑对原发灶进行切除/根治性RT以及对转移病灶进行切除,以改善生存结局。