Odackal John, Yu Victor, Gomez-Manjerres Diana, Field Joshua J, Burdick Marie D, Mehrad Borna
Dept of Medicine, University of Virginia School of Medicine, Charlottesville, VA, USA.
Division of Pulmonary, Critical Care, and Sleep Medicine, University of Florida, Gainesville, FL, USA.
ERJ Open Res. 2020 Nov 10;6(4). doi: 10.1183/23120541.00481-2020. eCollection 2020 Oct.
Autoimmunity is a common cause of pulmonary fibrosis and can present either as a manifestation of an established connective tissue disease or as the recently described entity of interstitial pneumonia with autoimmune features. The rate of progression and responsiveness to immunosuppression in these illnesses are difficult to predict. Circulating fibrocytes are bone marrow-derived progenitor cells that home to injured tissues and contribute to lung fibrogenesis. We sought to test the hypothesis that the blood fibrocyte concentration predicts outcome and treatment responsiveness in autoimmune interstitial lung diseases.
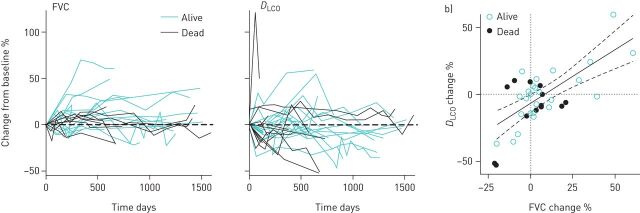
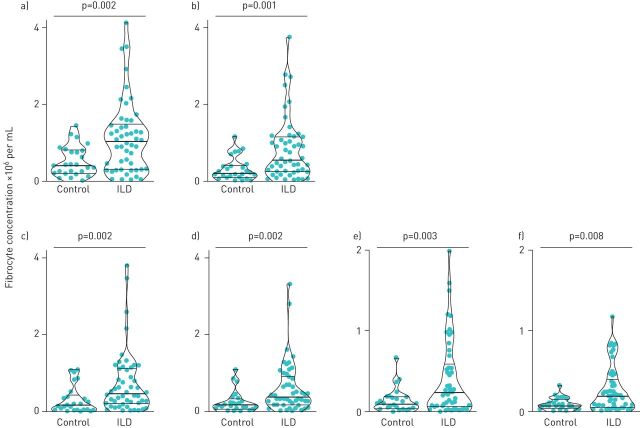
We compared the concentration of circulating fibrocytes in 50 subjects with autoimmune interstitial lung disease and 26 matched healthy controls and assessed the relationship between serial peripheral blood fibrocyte concentrations and clinical outcomes over a median of 6.25 years.
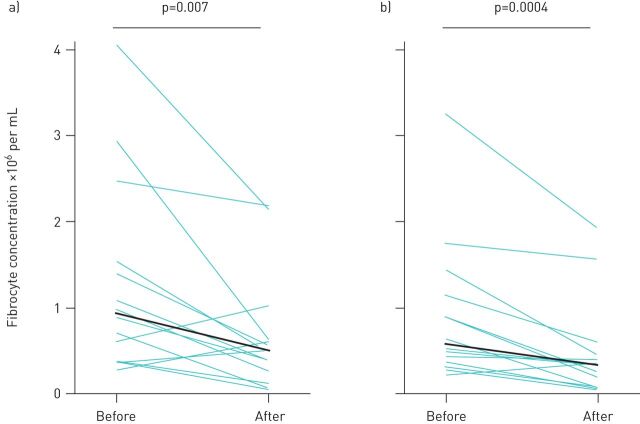
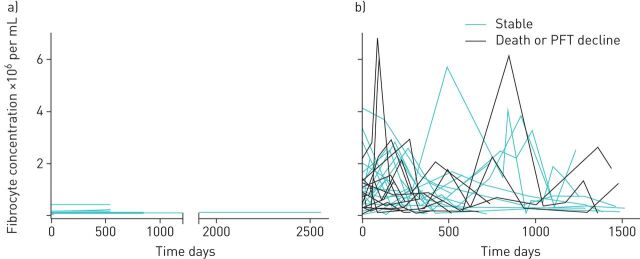
As compared to controls, subjects with autoimmune interstitial lung disease had higher circulating concentrations of total fibrocytes, the subset of activated fibrocytes, and fibrocytes with activation of PI3K/AKT/mTOR, transforming growth factor-β (TGF-β) receptor and interleukin (IL)-4/IL-13 receptor signalling pathways. Over the follow-up period, there were episodes of marked elevation in the concentration of circulating fibrocytes in subjects with autoimmune interstitial lung disease but not controls. Initiation of immunosuppressive therapy was associated with a decline in the concentration of circulating fibrocytes. For each 100 000 cells·mL increase in peak concentration of circulating fibrocytes, we found a 5% increase in odds of death or lung function decline.
In patients with autoimmune interstitial lung disease, circulating fibrocytes may represent a biomarker of outcome and treatment response.
自身免疫是肺纤维化的常见病因,可表现为已确诊的结缔组织病的一种表现形式,或表现为最近描述的具有自身免疫特征的间质性肺炎。这些疾病的进展速度和对免疫抑制的反应性难以预测。循环纤维细胞是源自骨髓的祖细胞,可归巢至受损组织并促进肺纤维化形成。我们试图验证以下假设:血液中纤维细胞浓度可预测自身免疫性间质性肺病的预后和治疗反应性。
我们比较了50例自身免疫性间质性肺病患者和26例匹配的健康对照者的循环纤维细胞浓度,并评估了连续外周血纤维细胞浓度与中位时间为6.25年的临床结局之间的关系。
与对照组相比,自身免疫性间质性肺病患者的总纤维细胞、活化纤维细胞亚群以及PI3K/AKT/mTOR、转化生长因子-β(TGF-β)受体和白细胞介素(IL)-4/IL-13受体信号通路激活的纤维细胞的循环浓度更高。在随访期间,自身免疫性间质性肺病患者的循环纤维细胞浓度有明显升高的情况,但对照组没有。免疫抑制治疗的开始与循环纤维细胞浓度的下降有关。循环纤维细胞峰值浓度每增加100 000个·mL,我们发现死亡或肺功能下降的几率增加5%。
在自身免疫性间质性肺病患者中,循环纤维细胞可能代表预后和治疗反应的生物标志物。