Auckland Diabetes Centre, Auckland City Hospital, Auckland, Aotearoa-New Zealand
Faculty of Medical and Health Sciences, The University of Auckland, Auckland, Aotearoa-New Zealand.
BMJ Open Diabetes Res Care. 2020 Dec;8(2). doi: 10.1136/bmjdrc-2020-001837.
In people accepted onto a bariatric surgery program we compared diabetes-related outcomes in those who completed surgery with those who withdrew before having surgery-examining rates of insulin use in people with type 2 diabetes (T2D), and rates of incident diabetes in people without pre-existing T2D.
771 people were accepted onto the program. 463 people (60%) had T2D at referral, of which 48% completed surgery and 52% withdrew. Of 308 people without T2D at referral, 49% completed surgery, and 51% withdrew. Rates of insulin use and incident diabetes were compared by Kaplan-Meier analyses. Among those with pre-existing T2D, we examined rates of remission and relapse after surgery.
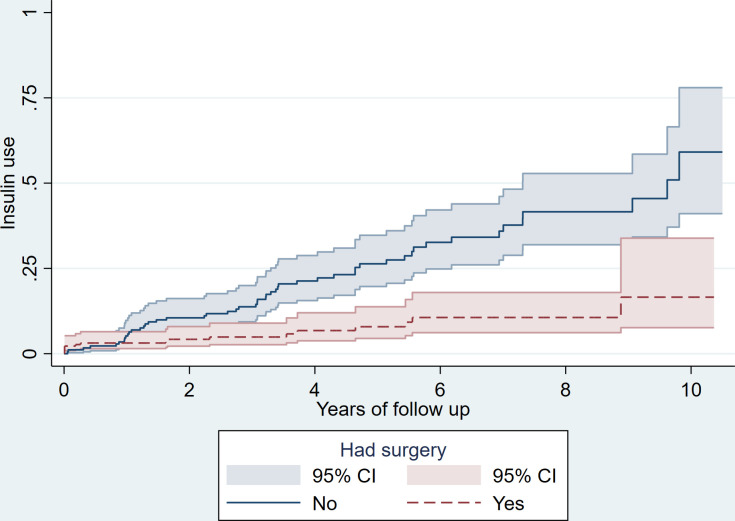
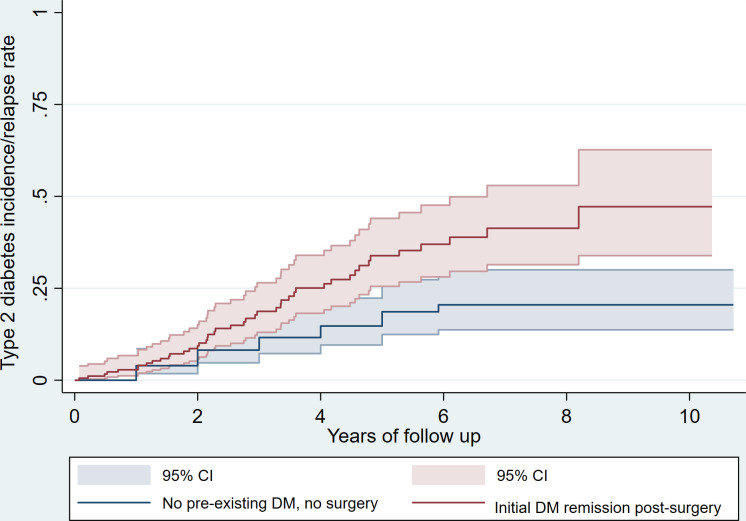
People without T2D who withdrew from the program had higher mean body mass index and glycated hemoglobin levels than those completing surgery (p<0.005). The rate of incident diabetes at 5 years was 19% in those who withdrew versus 0% in those completing surgery (p<0.001). 30% of people with T2D were taking insulin at referral and all stopped insulin after surgery. During follow-up, the rate of insulin (re)introduction was lower in those who completed surgery (8% vs 26% at 5 years, p<0.001). Of those with T2D who completed surgery, 80% had remission, but 34% had relapsed by 5 years. Diabetes relapse was associated with less weight loss after surgery, a longer duration of T2D and previous insulin use.
Despite a high relapse rate, people with T2D who completed surgery had lower insulin use at 5 years than those withdrawing from the program. In people without T2D, bariatric surgery prevented incident diabetes. People without T2D who withdrew from the program were at greater risk of diabetes, suggesting those who could benefit the most in terms of T2D prevention are not completing bariatric surgery.
在接受减重手术项目的人群中,我们比较了已完成手术和未手术前退出手术的患者的糖尿病相关结局——检查 2 型糖尿病(T2D)患者的胰岛素使用率,以及无既往 T2D 的新发糖尿病率。
771 人被纳入该项目。463 人(60%)在转介时患有 T2D,其中 48%完成手术,52%退出。308 人在转介时无 T2D,其中 49%完成手术,51%退出。通过 Kaplan-Meier 分析比较胰岛素使用和新发糖尿病的发生率。在既往患有 T2D 的患者中,我们检查了手术后缓解和复发的发生率。
退出该项目的无 T2D 患者的平均体重指数和糖化血红蛋白水平高于完成手术的患者(p<0.005)。在退出组中,5 年内新发糖尿病的发生率为 19%,而在完成手术组中为 0%(p<0.001)。30%的 T2D 患者在转介时正在服用胰岛素,所有患者在手术后均停止使用胰岛素。在随访期间,完成手术的患者胰岛素(再)使用率较低(5 年内分别为 8%和 26%,p<0.001)。完成手术的 T2D 患者中有 80%缓解,但 5 年内有 34%复发。糖尿病复发与手术后体重减轻较少、T2D 持续时间较长和既往胰岛素使用有关。
尽管复发率较高,但完成手术的 T2D 患者在 5 年内的胰岛素使用量低于退出手术的患者。在无 T2D 的患者中,减重手术可预防新发糖尿病。退出该项目的无 T2D 患者发生糖尿病的风险更高,这表明那些最有可能从 T2D 预防中获益的患者并未完成减重手术。