Centro de Investigación en Ciencias de la Salud Anáhuac (CICSA), Facultad de Ciencias de la Salud, Universidad Anáhuac México, Huixquilucan, Estado de México, México.
Department of Medical Education and Research, ABC Medical Center, Mexico City, CDMX, Mexico.
PLoS One. 2020 Dec 3;15(12):e0243268. doi: 10.1371/journal.pone.0243268. eCollection 2020.
Early identification of different COVID-19 clinical presentations may depict distinct pathophysiological mechanisms and guide management strategies.
To determine the aggressiveness of SARS-CoV-2 using symptom progression in COVID-19 patients.
Historic cohort study of Mexican patients. Data from January-April 2020 were provided by the Health Ministry.
Population-based. Patients registered in the Epidemiologic Surveillance System in Mexico.
Subjects who sought medical attention for clinical suspicion of COVID-19. All patients were subjected to RT-PCR testing for SARS-CoV-2.
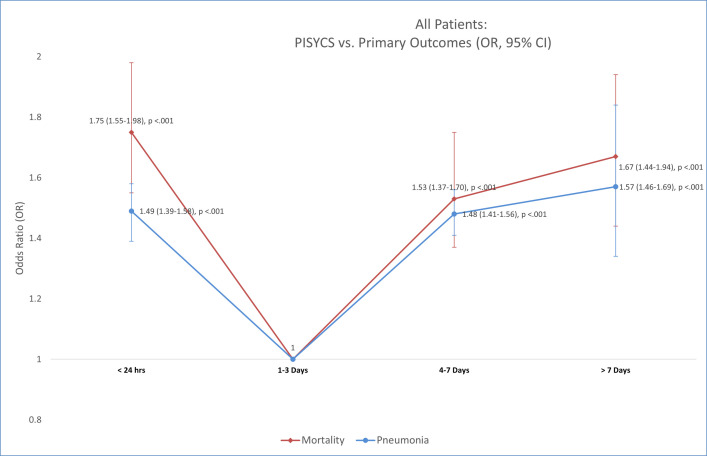
We measured the Period between initial symptoms and clinical progression to COVID-19 suspicion (PISYCS) and compared it to the primary outcomes (mortality and pneumonia).
65,500 patients were included. Reported fatalities and pneumonia were 2176 (3.32%), and 11568 (17.66%), respectively. According to the PISYCS, patients were distributed as follows: 14.89% in <24 hours, 43.25% between 1-3 days, 31.87% between 4-7 days and 9.97% >7 days. The distribution for mortality and pneumonia was 5.2% and 22.5% in <24 hours, 2.5% and 14% between 1-3 days, 3.6% and 19.5% between 4-7 days, 4.1% and 20.6% >7 days, respectively (p<0.001). Adjusted-risk of mortality was (OR [95% CI], p-value): <24 hours = 1.75 [1.55-1.98], p<0.001; 1-3 days = 1 (reference value); 4-7 days = 1.53 [1.37-1.70], p<0.001; >7 days = 1.67 [1.44-1.94], p<0.001. For pneumonia: <24 hours = 1.49 [1.39-1.58], p<0.001; 1-3 days = 1; 4-7 days = 1.48 [1.41-1.56], p<0.001; >7 days = 1.57 [1.46-1.69], p<0.001.
Using a database fed by large numbers of people carries the risk of data inaccuracy. However, this imprecision is expected to be random and data are consistent with previous studies.
The PISYCS shows a U-shaped SARS-CoV-2 aggressiveness pattern. Further studies are needed to corroborate the time-related pathophysiology behind these findings.
早期识别不同的 COVID-19 临床表现可能描绘出不同的病理生理机制,并指导管理策略。
使用 COVID-19 患者症状进展来确定 SARS-CoV-2 的侵袭性。
墨西哥患者的历史性队列研究。2020 年 1 月至 4 月的数据由卫生部提供。
基于人群。在墨西哥登记的流行病学监测系统中的患者。
因临床疑似 COVID-19 而寻求医疗关注的受试者。所有患者均接受 SARS-CoV-2 的 RT-PCR 检测。
我们测量了从最初症状到 COVID-19 疑似(PISYCS)的时间间隔,并将其与主要结局(死亡率和肺炎)进行了比较。
共纳入 65500 例患者。报告的死亡率和肺炎分别为 2176(3.32%)和 11568(17.66%)。根据 PISYCS,患者分布如下:<24 小时为 14.89%,1-3 天为 43.25%,4-7 天为 31.87%,>7 天为 9.97%。死亡率和肺炎的分布为:<24 小时为 5.2%和 22.5%,1-3 天为 2.5%和 14%,4-7 天为 3.6%和 19.5%,>7 天为 4.1%和 20.6%,分别为(p<0.001)。调整后的死亡率风险(OR [95%CI],p 值)为:<24 小时=1.75 [1.55-1.98],p<0.001;1-3 天=1(参考值);4-7 天=1.53 [1.37-1.70],p<0.001;>7 天=1.67 [1.44-1.94],p<0.001。对于肺炎:<24 小时=1.49 [1.39-1.58],p<0.001;1-3 天=1;4-7 天=1.48 [1.41-1.56],p<0.001;>7 天=1.57 [1.46-1.69],p<0.001。
使用由大量人群提供的数据的数据库存在数据不准确的风险。然而,这种不准确性预计是随机的,并且数据与先前的研究一致。
PISYCS 显示 SARS-CoV-2 侵袭性呈 U 形模式。需要进一步的研究来证实这些发现背后的时间相关病理生理学。