Khan Danyal Z, Placek Michal M, Smielewski Peter, Budohoski Karol P, Anwar Fahim, Hutchinson Peter J A, Bance Manohar, Czosnyka Marek, Helmy Adel
Division of Neurosurgery, University of Cambridge and Cambridge University Hospitals NHS Foundation Trust, Cambridge, United Kingdom.
Brain Physics Laboratory, Department of Clinical Neurosciences, University of Cambridge, Cambridge, United Kingdom.
Neurotrauma Rep. 2020 Nov 25;1(1):218-231. doi: 10.1089/neur.2020.0021. eCollection 2020.
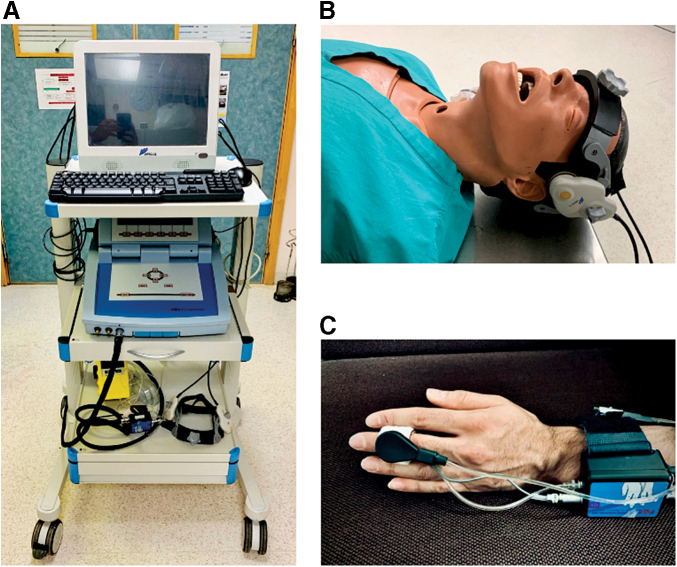
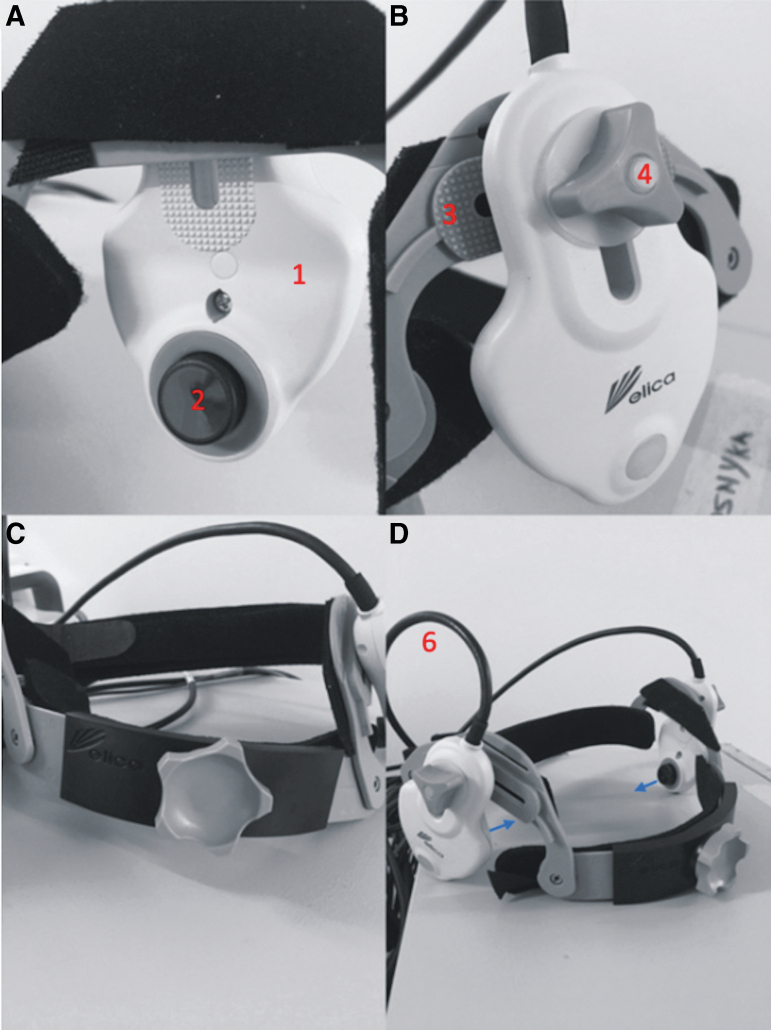
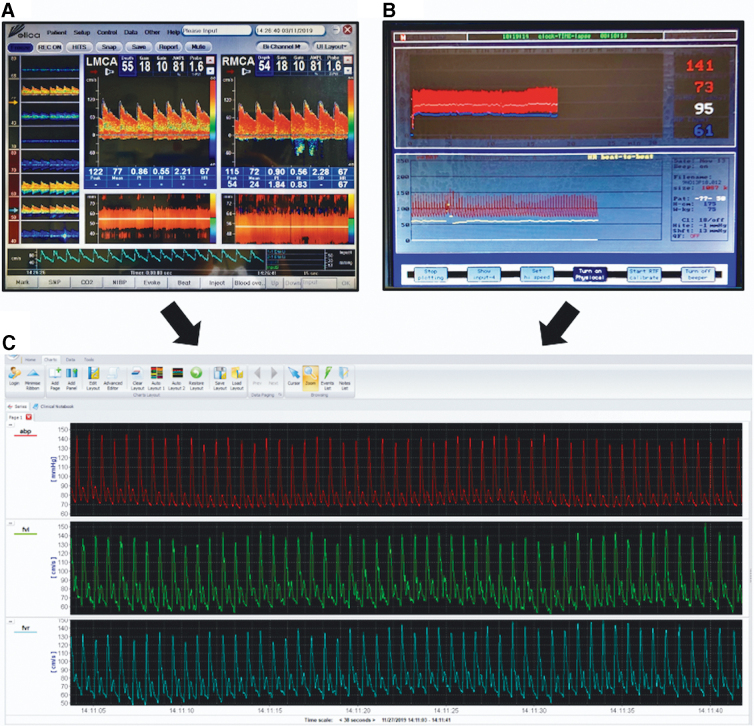
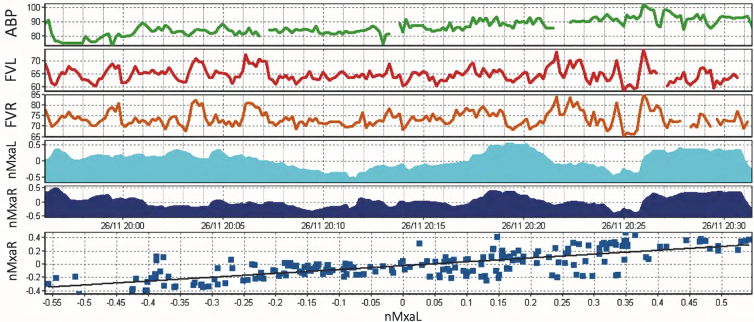
Post-concussion syndrome (PCS) refers to a constellation of physical, cognitive, and emotional symptoms after traumatic brain injury (TBI). Despite its incidence and impact, the underlying mechanisms of PCS are unclear. We hypothesized that impaired cerebral autoregulation (CA) is a contributor. In this article, we present our protocol for non-invasively assessing CA in patients with TBI and PCS in a real-world clinical setting. A prospective, observational study was integrated into outpatient clinics at a tertiary neurosurgical center. Data points included: demographics, symptom profile (Post-Concussion Symptom Scale [PCSS]) and neuropsychological assessment (Cambridge Neuropsychological Test Automated-Battery [CANTAB]). Cerebrovascular metrics (nMxa co-efficient and the transient hyperaemic-response ratio [THRR]) were collected using transcranial Doppler (TCD), finger plethysmography, and bespoke software (ICM+). Twelve participants were initially recruited but 2 were excluded after unsuccessful insonation of the middle cerebral artery (MCA); 10 participants (5 patients with TBI, 5 healthy controls) were included in the analysis (median age 26.5 years, male to female ratio: 7:3). Median PCSS scores were 6/126 for the TBI patient sub-groups. Median CANTAB percentiles were 78 (healthy controls) and 25 (TBI). nMxa was calculated for 90% of included patients, whereas THRR was calculated for 50%. Median study time was 127.5 min and feedback ( = 6) highlighted the perceived acceptability of the study. This pilot study has demonstrated a reproducible assessment of PCS and CA metrics (non-invasively) in a real-world setting. This protocol is feasible and is acceptable to participants. By scaling this methodology, we hope to test whether CA changes are correlated with symptomatic PCS in patients post-TBI.
脑震荡后综合征(PCS)是指创伤性脑损伤(TBI)后出现的一系列身体、认知和情感症状。尽管其发病率和影响较大,但PCS的潜在机制尚不清楚。我们假设脑自动调节(CA)受损是一个促成因素。在本文中,我们介绍了在真实临床环境中对TBI和PCS患者进行CA无创评估的方案。一项前瞻性观察性研究纳入了一家三级神经外科中心的门诊诊所。数据点包括:人口统计学、症状概况(脑震荡后症状量表[PCSS])和神经心理学评估(剑桥神经心理测试自动成套测验[CANTAB])。使用经颅多普勒(TCD)、手指体积描记法和定制软件(ICM+)收集脑血管指标(nMxa系数和瞬时充血反应比[THRR])。最初招募了12名参与者,但在大脑中动脉(MCA)探测失败后排除了2名;分析纳入了10名参与者(5名TBI患者,5名健康对照)(中位年龄26.5岁,男女比例:7:3)。TBI患者亚组的PCSS中位数为6/126。CANTAB百分位数中位数在健康对照中为78,在TBI患者中为25。90%的纳入患者计算了nMxa,而50%的患者计算了THRR。中位研究时间为127.5分钟,反馈(=6)突出了该研究的可接受性。这项初步研究在真实环境中证明了对PCS和CA指标(无创)的可重复评估。该方案可行且参与者可接受。通过扩大这种方法的规模,我们希望测试TBI后患者的CA变化是否与有症状的PCS相关。