Christidi Aikaterini, Haschemi Jafer, Spieker Maximilian, Bönner Florian, Kelm Malte, Westenfeld Ralf, Horn Patrick
Division of Cardiology, Pulmonology, and Vascular Medicine, Medical Faculty, Heinrich Heine University, Düsseldorf, Germany.
Cardiovascular Research Institute, Medical Faculty, Heinrich Heine University Düsseldorf, Düsseldorf, Germany.
ESC Heart Fail. 2021 Feb;8(1):577-585. doi: 10.1002/ehf2.13127. Epub 2020 Dec 6.
Percutaneous mitral valve repair (PMVR) has emerged as standard treatment in selected patients with clinically relevant mitral regurgitation (MR) and increased surgical risk. We aimed to evaluate the safety and clinical outcomes in nonagenarians undergoing PMVR.
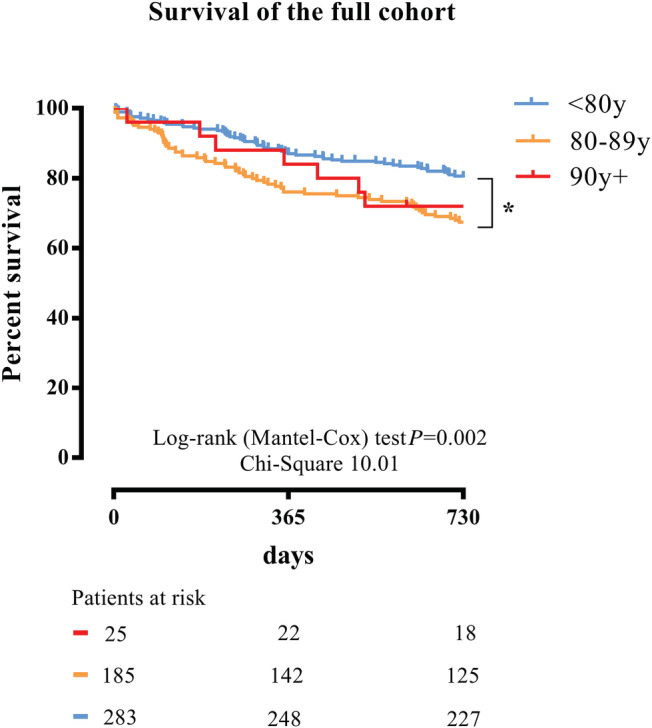
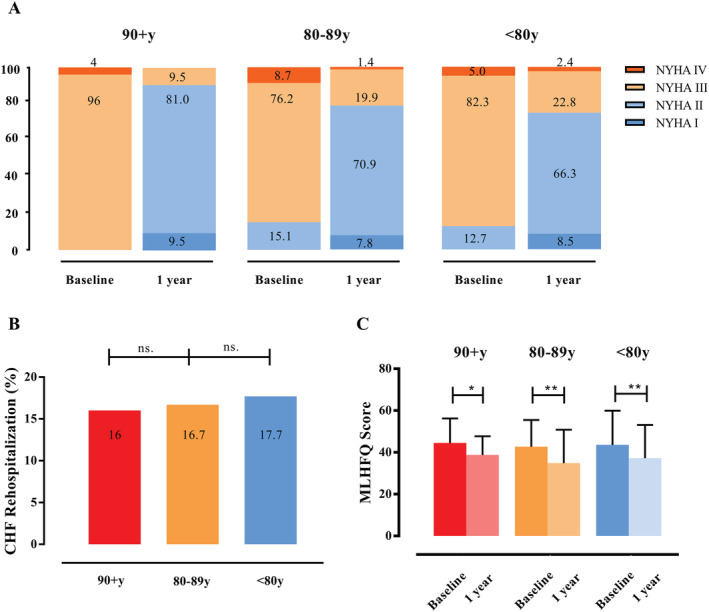
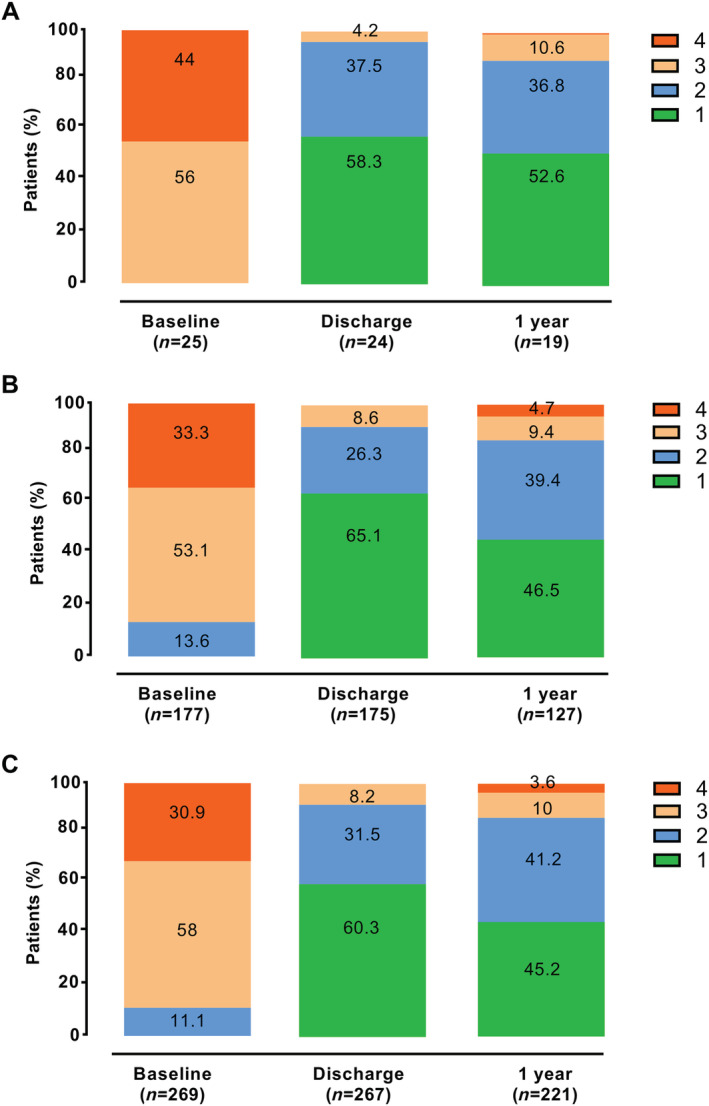
Altogether, 493 patients with severe MR who were treated with PMVR were included in this open-label prospective study and followed up for 2 years. We treated 25 patients with PMVR aged 90 years or above, 185 patients aged 80-89 years, and 283 patients aged <80 years. PMVR in nonagenarians was safe and did not differ from PMVR in younger patients in terms of safety endpoints. Device success did not differ among the groups (100% in nonagenarians, 95.7% in octogenarians, and 95.1% in septuagenarians, P = 0.100). Unadjusted 2 year mortality was 28% in nonagenarians, 32.4% in octogenarians, and 19.8% in septuagenarians (P = 0.008). Kaplan-Meier curves confirmed similar 2 year survival in the nonagenarian and octogenarian groups (P = 0.657). In the multivariate analysis, age [hazard ratio (HR) 1.031, 95% confidence interval (CI) 1.002-1.060, P = 0.034], higher post-procedural transmitral valve gradients (HR 1.187, 95% CI 1.104-1.277, P = 0.001), and post-procedural acute kidney injury (HR 2.360, 95% CI 1.431-3.893, P = 0.001) were independent predictors of 2 year mortality. Altogether, 89.4% of the nonagenarians, 85.9% of the octogenarians, and 86.4% of the septuagenarians had MR grade of 2+ or less at 1 year after PMVR (P = 0.910). New York Heart Association functional class improved in the vast majority of patients, irrespective of age (P = 0.129). After 1 year, 9.5% of the nonagenarians, 22.3% of the octogenarians, and 25.2% of the septuagenarians (each P = 0.001 compared with baseline) suffered from New York Heart Association Functional Class III or IV. The rate of heart failure rehospitalization in the first 12 months after PMVR did not differ among the groups (16% in the nonagenarians, 16.7% in the octogenarians, and 17.7% in the septuagenarians) (P = 0.954). Quality of life assessed by the Minnesota Living with Heart Failure Questionnaire before and at 1 year after PMVR improved in all age groups (P = 0.001).
Percutaneous mitral valve repair in carefully selected nonagenarians is feasible and safe with intermediate-term beneficial effects comparable with those in younger patients.
经皮二尖瓣修复术(PMVR)已成为部分有临床意义的二尖瓣反流(MR)且手术风险增加患者的标准治疗方法。我们旨在评估90岁及以上患者接受PMVR的安全性和临床结局。
本开放标签前瞻性研究共纳入493例接受PMVR治疗的重度MR患者,并进行了2年的随访。我们治疗了25例年龄在90岁及以上的PMVR患者、185例年龄在80 - 89岁的患者以及283例年龄小于80岁的患者。90岁及以上患者的PMVR是安全的,在安全终点方面与年轻患者的PMVR没有差异。各组间器械成功率无差异(90岁及以上患者为100%,80岁患者为95.7%,70岁患者为95.1%,P = 0.100)。未经调整的2年死亡率在90岁及以上患者中为28%,80岁患者中为32.4%,70岁患者中为19.8%(P = 0.008)。Kaplan-Meier曲线证实90岁及以上患者组和80岁患者组2年生存率相似(P = 0.657)。多因素分析中,年龄[风险比(HR)1.031,95%置信区间(CI)1.002 - 1.060,P = 0.034]、术后二尖瓣跨瓣压差升高(HR 1.187,95% CI 1.104 - 1.277,P = 0.001)以及术后急性肾损伤(HR 2.360,95% CI 1.431 - 3.893,P = 0.001)是2年死亡率的独立预测因素。总体而言,90岁及以上患者中89.4%、80岁患者中85.9%、70岁患者中86.4%在PMVR术后1年时MR分级为2+或更低(P = 0.910)。绝大多数患者的纽约心脏协会(NYHA)心功能分级得到改善,与年龄无关(P = 0.129)。1年后,90岁及以上患者中有9.5%、80岁患者中有22.3%、70岁患者中有25.2%(与基线相比,每组P = 0.001)出现NYHA心功能Ⅲ级或Ⅳ级。PMVR术后前12个月内心力衰竭再住院率在各组间无差异(90岁及以上患者为16%,80岁患者为16.7%,70岁患者为17.7%)(P = 0.954)。通过明尼苏达心力衰竭生活问卷评估的生活质量在PMVR术前及术后1年时在所有年龄组中均有所改善(P = 0.001)。
在精心挑选的90岁及以上患者中,经皮二尖瓣修复术是可行且安全的,中期有益效果与年轻患者相当。