Wei Yousheng, Ou Tingyu, Lu Yan, Wu Guangteng, Long Ying, Pan Xinbin, Yao Desheng
Department of Gynecologic Oncology, Guangxi Medical University Cancer Hospital, Nanning, Guangxi, China.
Department of Radiation Oncology, Guangxi Medical University Cancer Hospital, Nanning, Guangxi, China.
PeerJ. 2020 Nov 24;8:e10414. doi: 10.7717/peerj.10414. eCollection 2020.
Ovarian cancer is a highly fatal gynecological malignancy and new, more effective treatments are needed. Immunotherapy is gaining attention from researchers worldwide, although it has not proven to be consistently effective in the treatment of ovarian cancer. We studied the immune landscape of ovarian cancer patients to improve the efficacy of immunotherapy as a treatment option.
We obtained expression profiles, somatic mutation data, and clinical information from The Cancer Genome Atlas. Ovarian cancer was classified based on 29 immune-associated gene sets, which represented different immune cell types, functions, and pathways. Single-sample gene set enrichment (ssGSEA) was used to quantify the activity or enrichment levels of the gene sets in ovarian cancer, and the unsupervised machine learning method was used sort the classifications. Our classifications were validated using Gene Expression Omnibus datasets.
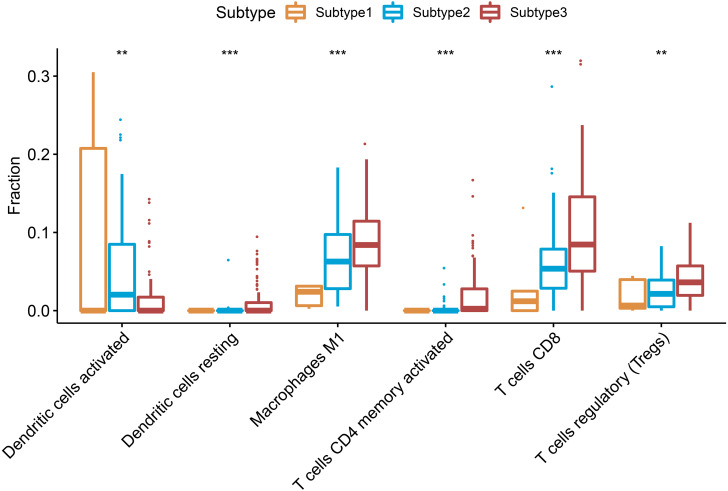
We divided ovarian cancer into three subtypes according to the ssGSEA score: subtype 1 (low immunity), subtype 2 (median immunity), and subtype 3 (high immunity). Most tumor-infiltrating immune cells and immune checkpoint molecules were upgraded in subtype 3 compared with those in the other subtypes. The tumor mutation burden (TMB) was not significantly different among the three subtypes. However, patients with BRCA1 mutations were consistently detected in subtype 3. Furthermore, most immune signature pathways were hyperactivated in subtype 3, including T and B cell receptor signaling pathways, PD-L1 expression and PD-1 checkpoint pathway the NF-B signaling pathway, Th17 cell differentiation and interleukin-17 signaling pathways, and the TNF signaling pathway.
Ovarian cancer subtypes that are based on immune biosignatures may contribute to the development of novel therapeutic treatment strategies for ovarian cancer.
卵巢癌是一种极具致死性的妇科恶性肿瘤,需要新的、更有效的治疗方法。免疫疗法正受到全球研究人员的关注,尽管它尚未被证明在卵巢癌治疗中始终有效。我们研究了卵巢癌患者的免疫格局,以提高免疫疗法作为一种治疗选择的疗效。
我们从癌症基因组图谱中获取了表达谱、体细胞突变数据和临床信息。根据29个免疫相关基因集对卵巢癌进行分类,这些基因集代表不同的免疫细胞类型、功能和途径。采用单样本基因集富集分析(ssGSEA)来量化基因集在卵巢癌中的活性或富集水平,并使用无监督机器学习方法对分类进行排序。我们的分类使用基因表达综合数据库进行了验证。
根据ssGSEA评分,我们将卵巢癌分为三个亚型:亚型1(低免疫)、亚型2(中等免疫)和亚型3(高免疫)。与其他亚型相比,亚型3中的大多数肿瘤浸润免疫细胞和免疫检查点分子水平有所升高。三个亚型之间的肿瘤突变负荷(TMB)没有显著差异。然而,在亚型3中持续检测到携带BRCA1突变的患者。此外,大多数免疫特征途径在亚型3中过度激活,包括T和B细胞受体信号通路、PD-L1表达和PD-1检查点途径、NF-κB信号通路、Th17细胞分化和白细胞介素-17信号通路以及TNF信号通路。
基于免疫生物标志物的卵巢癌亚型可能有助于开发卵巢癌的新型治疗策略。