Chen Fangming, Zhou Yongping, Qi Xiumin, Zhang Rui, Gao Xin, Xia Wei, Zhang Lei
Department of Radiology, The Affiliated Wuxi No.2 People's Hospital of Nanjing Medical University, Wuxi, China.
Department of Hepatobiliary Surgery, The Affiliated Wuxi No.2 People's Hospital of Nanjing Medical University, Wuxi, China.
Front Oncol. 2020 Nov 16;10:523543. doi: 10.3389/fonc.2020.523543. eCollection 2020.
To develop a radiomics signature for predicting surgical portal vein-superior mesenteric vein (PV-SMV) in patients with pancreatic ductal adenocarcinoma (PDAC) and measure the effect of providing the predictions of radiomics signature to radiologists with different diagnostic experiences during imaging interpretation.
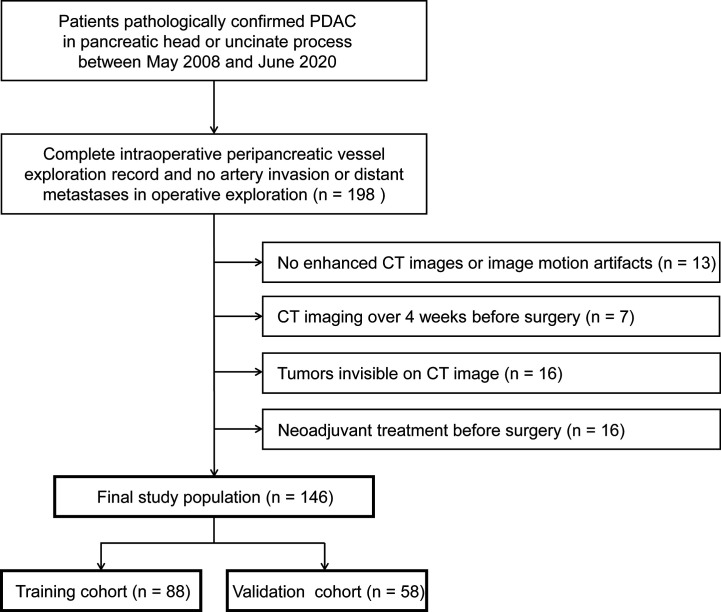
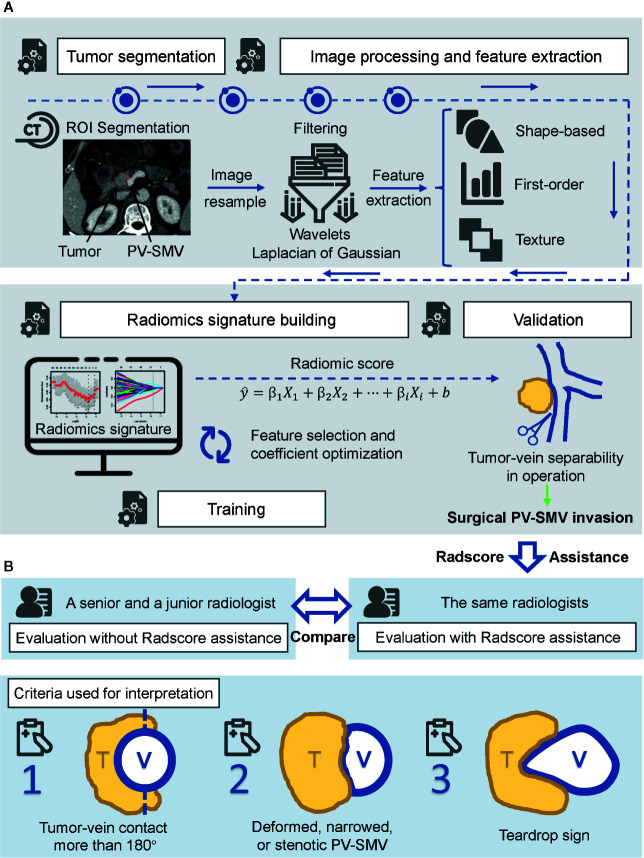
Between February 2008 and June 2020, 146 patients with PDAC in pancreatic head or uncinate process from two institutions were retrospectively included and randomly split into a training (n = 88) and a validation (n =58) cohort. Intraoperative vascular exploration findings were used to identify surgical PV-SMV invasion. Radiomics features were extracted from the portal venous phase CT images. Radiomics signature was built with a linear elastic-net regression model. Area under receiver operating characteristic curve (AUC) of the radiomics signature was calculated. A senior and a junior radiologist independently review CT scans and made the diagnosis for PV-SMV invasion both with and without radiomics score (Radscore) assistance. A 2-sided Pearson's chi-squared test was conducted to evaluate whether there was a difference in sensitivity, specificity, and accuracy between the radiomics signature and the unassisted radiologists. To assess the incremental value of providing Radscore predictions to the radiologists, we compared the performance between unassisted evaluation and Radscore-assisted evaluation by using the McNemar test.
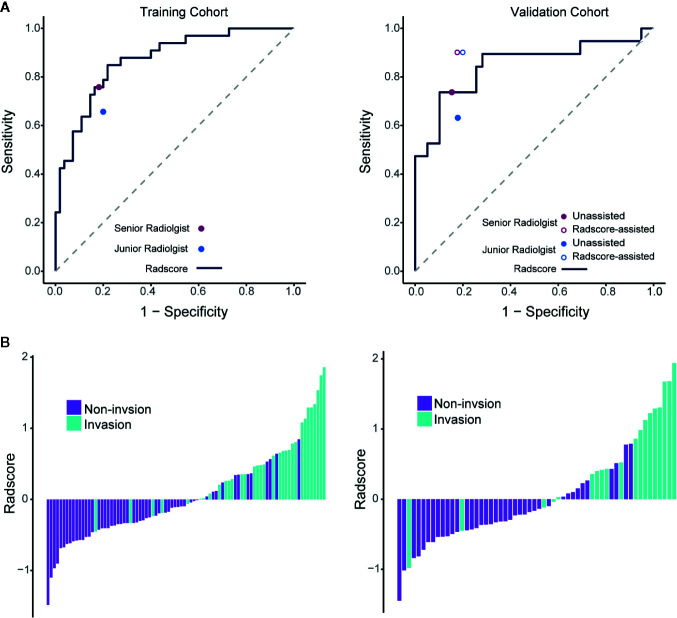
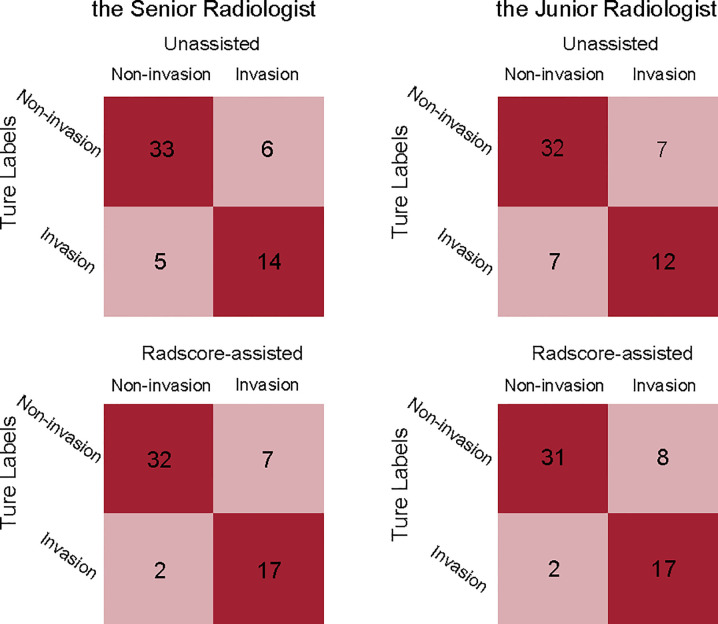
Numbers of patients identified as presence of surgical PV-SMV invasion were 33 (37.5%) and 19 (32.8%) in the training and validation cohort, respectively. The radiomics signature achieved an AUC of 0.848 (95% confidence interval, 0.724-0.971) in the validation cohort and had a comparable sensitivity, specificity, and accuracy as the senior radiologist in predicting PV-SMV invasion (all -values > 0.05). Providing predictions of radiomics signature increased both radiologists' sensitivity in identifying PV-SMV invasion, while only the increase of the junior radiologist was significant (63.2 vs 89.5%, -value = 0.025) instead of the senior radiologist (73.7 vs 89.5%, -value = 0.08). Both radiologists' accuracy had no significant increase when provided radiomics signature assistance (both -values > 0.05).
The radiomics signature can predict surgical PV-SMV invasion in patients with PDAC and may have incremental value to the diagnostic performance of radiologists during imaging interpretation.
建立一种用于预测胰腺导管腺癌(PDAC)患者手术门静脉-肠系膜上静脉(PV-SMV)侵犯的影像组学特征,并评估在影像解读过程中为具有不同诊断经验的放射科医生提供影像组学特征预测的效果。
回顾性纳入2008年2月至2020年6月期间来自两家机构的146例胰头或钩突部PDAC患者,并将其随机分为训练队列(n = 88)和验证队列(n = 58)。术中血管探查结果用于确定手术PV-SMV侵犯情况。从门静脉期CT图像中提取影像组学特征。使用线性弹性网络回归模型构建影像组学特征。计算影像组学特征的受试者操作特征曲线下面积(AUC)。一名资深放射科医生和一名初级放射科医生分别独立阅片,并在有无影像组学评分(Radscore)辅助的情况下对PV-SMV侵犯进行诊断。进行双侧Pearson卡方检验,以评估影像组学特征与未辅助的放射科医生在敏感性、特异性和准确性方面是否存在差异。为评估向放射科医生提供Radscore预测的增量价值,我们使用McNemar检验比较了未辅助评估和Radscore辅助评估之间的性能。
训练队列和验证队列中被确定存在手术PV-SMV侵犯的患者数量分别为33例(37.5%)和19例(32.8%)。影像组学特征在验证队列中的AUC为0.848(95%置信区间,0.724 - 0.971),在预测PV-SMV侵犯方面与资深放射科医生具有相当的敏感性、特异性和准确性(所有P值>0.05)。提供影像组学特征预测提高了两位放射科医生识别PV-SMV侵犯的敏感性,而只有初级放射科医生的提高具有显著性(63.2%对89.5%,P值 = 0.025),资深放射科医生则无显著性提高(73.7%对89.5%,P值 = 0.08)。在提供影像组学特征辅助时,两位放射科医生的准确性均无显著提高(两个P值>0.05)。
影像组学特征可预测PDAC患者手术PV-SMV侵犯,且在影像解读过程中可能对放射科医生诊断性能具有增量价值。