Jahreiß Marie-Christina, Aben Katja K H, Hoogeman Mischa S, Dirkx Maarten L P, de Vries Kim C, Incrocci Luca, Heemsbergen Wilma D
Department of Radiotherapy, Erasmus MC Cancer Institute, Rotterdam, Netherlands.
Department of Research & Development, Netherlands Comprehensive Cancer Organization, Utrecht, Netherlands.
Front Oncol. 2020 Nov 13;10:605119. doi: 10.3389/fonc.2020.605119. eCollection 2020.
Concerns have been raised that modern intensity modulated radiotherapy (IMRT) may be associated with increased second primary cancer risks (SPC) compared to previous three-dimensional conformal radiation techniques (3DCRT), due to increased low dose volumes and more out-of-field ionizing dose to peripheral tissue further away from the target. We assessed the impact of treatment technique on SPC risks in a cohort of prostate cancer (PCa) survivors.
The study cohort comprised 1,561 PCa survivors aged 50-79 years at time of radiotherapy, treated between 2006-2013 (N=707 IMRT, N=854 3DCRT). Treatment details were extracted from radiotherapy systems and merged with longitudinal data of the Netherlands Cancer Registry to identify SPCs. Primary endpoint was the development of a solid SPC (excluding skin cancer) in peripheral anatomical regions, i.e. non-pelvic. Applied latency period was 12 months. SPC rates in the IMRT cohort (total cohort and age subgroups) were compared to 1) the 3DCRT cohort by calculating Sub-Hazard Ratios (sHR) using a competing risk model, and 2) to the general male population by calculating Standardized Incidence Ratios (SIR). Models were adjusted for calendar period and age.
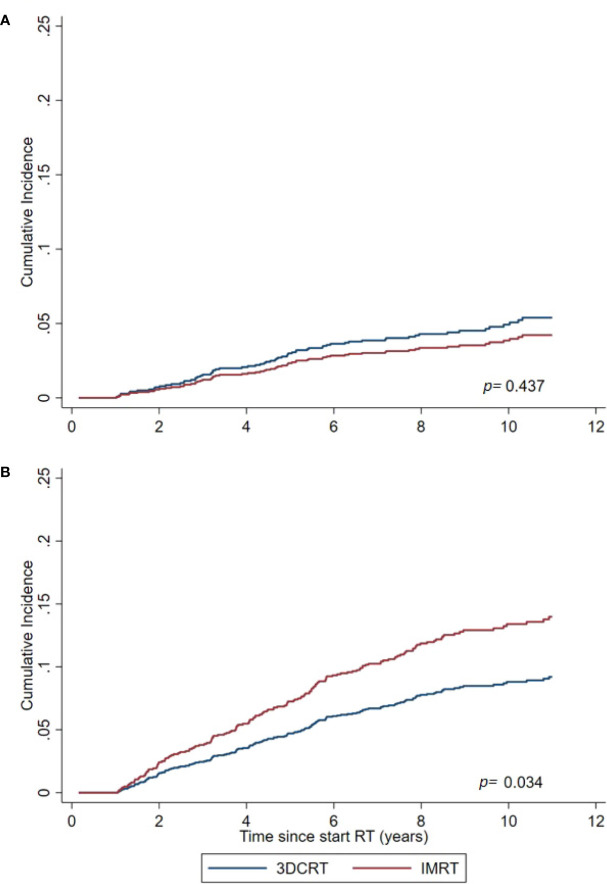
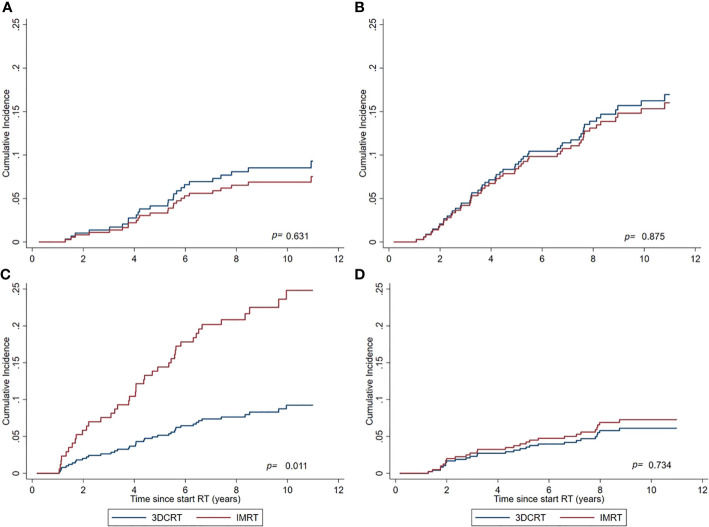
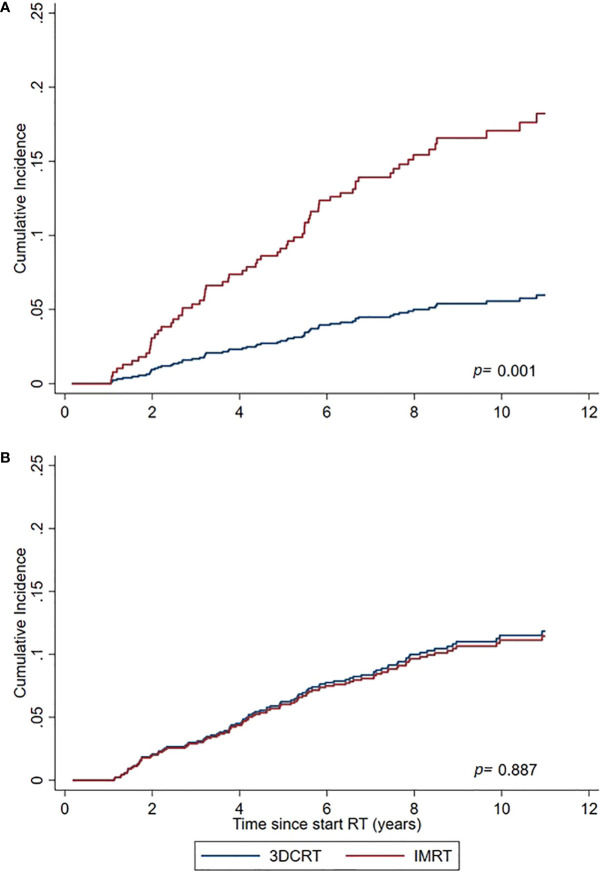
Median follow-up was 8.0 years (accumulated 11,664 person-years at-risk) with 159 cases developing ≥1 non-pelvic SPC. For IMRT vs 3DCRT we observed a significantly (=0.03) increased risk (sHR=1.56, 95% Confidence Interval (CI) 1.03-2.36, corresponding estimated excess absolute risk (EAR) of +7 cases per 10,000 person-years). At explorative analysis, IMRT was in particular associated with increased risks within the subgroup of active smokers (sHR 2.94, =0.01). Within the age subgroups 50-69 and 70-79 years, the sHR for non-pelvic SPC was 3.27 (=0.001) and 0.96 (=0.9), respectively. For pelvic SPC no increase was observed (sHR=0.8, 0.4). Compared to the general population, IMRT was associated with significantly increased risks for non-pelvic SPC in the 50-69 year age group (SIR=1.90, <0.05) but not in the 70-79 years group (SIR=1.08).
IMRT is associated with increased SPC risks for subjects who are relatively young at time of treatment. Additional research on aspects of IMRT that may cause this effect is essential to minimize risks for future patients receiving modern radiotherapy.
有人担心,与先前的三维适形放射技术(3DCRT)相比,现代调强放射治疗(IMRT)可能会增加第二原发性癌症风险(SPC),这是因为低剂量体积增加,且远离靶区的外周组织受到更多的野外电离辐射剂量。我们评估了治疗技术对一组前列腺癌(PCa)幸存者SPC风险的影响。
研究队列包括1561例放疗时年龄在50 - 79岁的PCa幸存者,他们于2006年至2013年接受治疗(N = 707例IMRT,N = 854例3DCRT)。从放疗系统中提取治疗细节,并与荷兰癌症登记处的纵向数据合并,以识别SPC。主要终点是外周解剖区域(即非盆腔)发生实体SPC(不包括皮肤癌)。应用的潜伏期为12个月。通过使用竞争风险模型计算亚危险比(sHR),将IMRT队列(总队列和年龄亚组)中的SPC发生率与1)3DCRT队列进行比较,并通过计算标准化发病比(SIR)与2)一般男性人群进行比较。模型针对日历期和年龄进行了调整。
中位随访时间为8.0年(累积11,664人年的风险),有159例发生≥1例非盆腔SPC。对于IMRT与3DCRT,我们观察到风险显著增加(P = 0.03)(sHR = 1.56,95%置信区间(CI)1.03 - 2.36,相应的估计绝对超额风险(EAR)为每10,000人年增加7例)。在探索性分析中,IMRT尤其与当前吸烟者亚组中的风险增加相关(sHR 2.94,P = 0.01)。在50 - 69岁和70 - 79岁年龄亚组中,非盆腔SPC的sHR分别为3.27(P = 0.001)和0.96(P = 0.9)。对于盆腔SPC,未观察到增加(sHR = 0.8,P = 0.4)。与一般人群相比,IMRT与50 - 69岁年龄组中非盆腔SPC的风险显著增加相关(SIR = 1.90,P < 0.05),但在70 - 79岁组中不相关(SIR = 1.08)。
IMRT与治疗时相对年轻的受试者的SPC风险增加相关。对IMRT可能导致这种效应的方面进行进一步研究对于将接受现代放疗的未来患者的风险降至最低至关重要。