Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, UK.
Obes Rev. 2021 Apr;22(4):e13151. doi: 10.1111/obr.13151. Epub 2020 Dec 6.
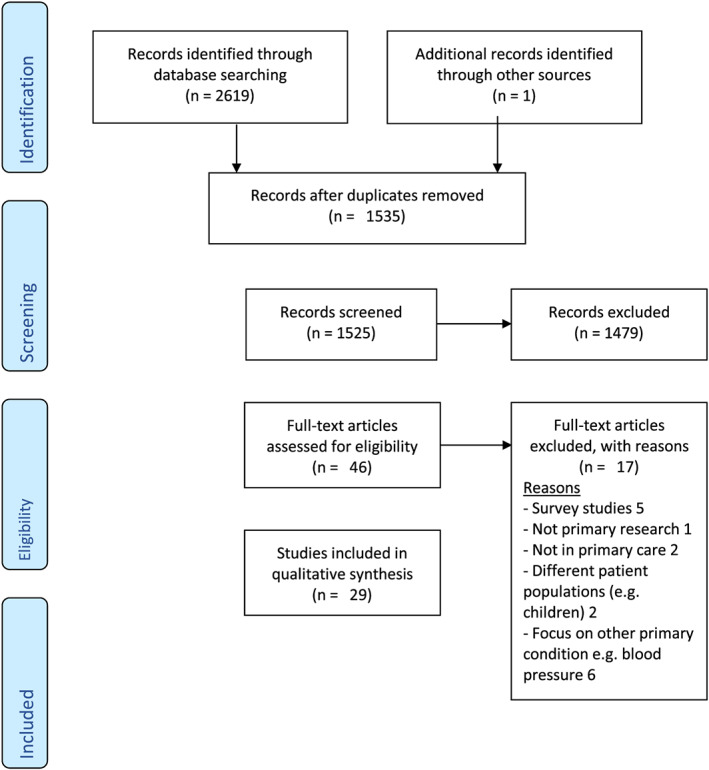
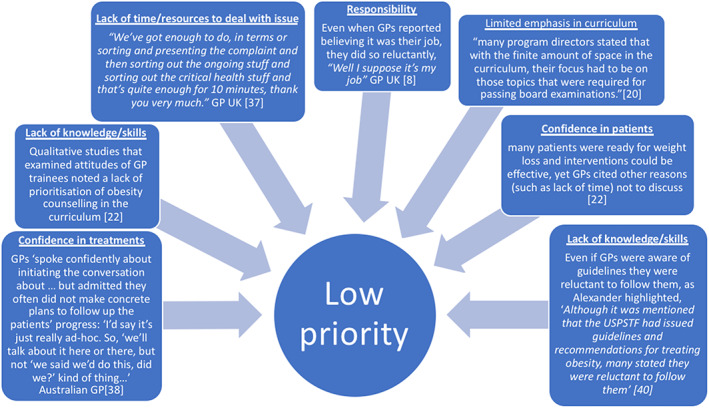
Guidelines and evidence suggest primary care clinicians should give opportunistic interventions to motivate weight loss, but these rarely occur in practice. We sought to examine why by systematically reviewing qualitative research examining general practitioners' ('GPs') and nurses' views of discussing weight with patients. We systematically searched English language publications (1945-2018) to identify qualitative interview and focus group studies. Thematic methods were used to synthesise the findings from these papers. We synthesised the studies by identifying second-order themes (explanations offered by the original researchers) and third-order constructs (new explanations which went beyond those in the original publications). Quality assessment using the Joanna Briggs checklist was undertaken. We identified 29 studies (>601 GPs, nurses and GP trainees) reporting views on discussing weight with patients. Key second-order themes were lack of confidence in treatments and patients' ability to make changes, stigma, interactional difficulty of discussing the topic and a belief of a wider societal responsibility needed to deal with patients with overweight and obesity. The third-order analytical theme was that discussions about weight were not a priority, and other behavioural interventions, including those relating to smoking, often took precedent. GPs and nurses reported that noting body mass index measurements at every consultation alongside a framework to deliver interventions would likely increase the frequency and perceived efficacy of behavioural weight interventions. GPs and nurses acknowledge the importance of obesity as a health issue, but this is insufficient, particularly amongst GPs, for them to construe this as a medical problem to address with patients in consultations. Strategies to implement clinical guidelines need to make tackling obesity a clinical priority. Training to overcome interactional difficulties, regular weighing of patients and changing expectations and understanding of weight loss interventions are also probably required.
指南和证据表明,初级保健临床医生应该提供机会性干预措施来激励体重减轻,但这些措施在实践中很少发生。我们通过系统地回顾检查全科医生('GP')和护士与患者讨论体重的观点的定性研究来探讨原因。我们系统地搜索了英语出版物(1945-2018 年),以确定定性访谈和焦点小组研究。使用主题方法综合这些论文的结果。我们通过识别二级主题(原始研究人员提供的解释)和三级结构(超越原始出版物的新解释)来综合研究。使用 Joanna Briggs 清单进行质量评估。我们确定了 29 项研究(>601 名全科医生、护士和全科医生实习生),报告了与患者讨论体重的观点。关键的二级主题是缺乏对治疗和患者改变能力的信心、耻辱感、讨论该主题的互动困难以及认为需要更广泛的社会责任感来应对超重和肥胖患者。第三个分析主题是,关于体重的讨论不是优先事项,其他行为干预措施,包括与吸烟有关的干预措施,通常优先考虑。全科医生和护士报告说,在每次就诊时记录体重指数测量值,并提供干预措施的框架,可能会增加行为体重干预的频率和感知效果。全科医生和护士承认肥胖是一个健康问题的重要性,但这还不够,特别是在全科医生中,不足以让他们将其视为与患者在咨询中解决的医疗问题。实施临床指南的策略需要将解决肥胖问题作为临床优先事项。克服互动困难的培训、定期为患者称重以及改变对减肥干预措施的期望和理解可能也是必要的。