Yang Kaili, Li Jiarui, Sun Zhao, Zhao Lin, Bai Chunmei
Department of Medical Oncology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing China.
Department of Medical Oncology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, No. 1 Shuai Fu Yuan, Dongcheng District, Beijing 100032, China.
Ther Adv Med Oncol. 2020 Nov 27;12:1758835920975353. doi: 10.1177/1758835920975353. eCollection 2020.
A large proportion of patients eventually experience disease progression despite treatment with immune checkpoint inhibitors (ICIs), but subsequent treatment options are limited for this population. Retreatment with the same or different types of ICIs is a possible strategy, but the clinical efficacy and safety data are limited. This systematic review aims to evaluate the efficacy and safety of ICIs retreatment in patients with solid tumors after disease progression to previous ICIs.
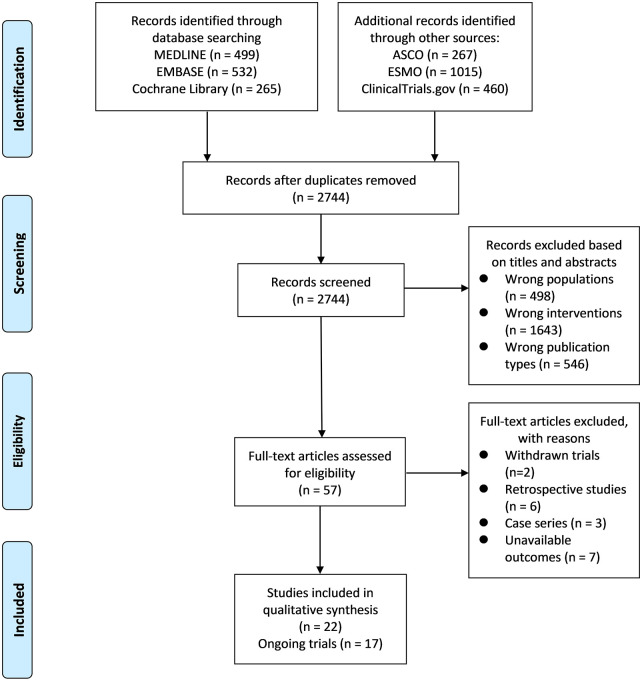
We searched MEDLINE, EMBASE, the Cochrane Library, and major meeting libraries for prospective studies. The primary outcomes included the objective response rate (ORR), disease control rate (DCR), median overall survival (mOS), and the incidence of grade ⩾3 immune-related adverse events (irAEs).
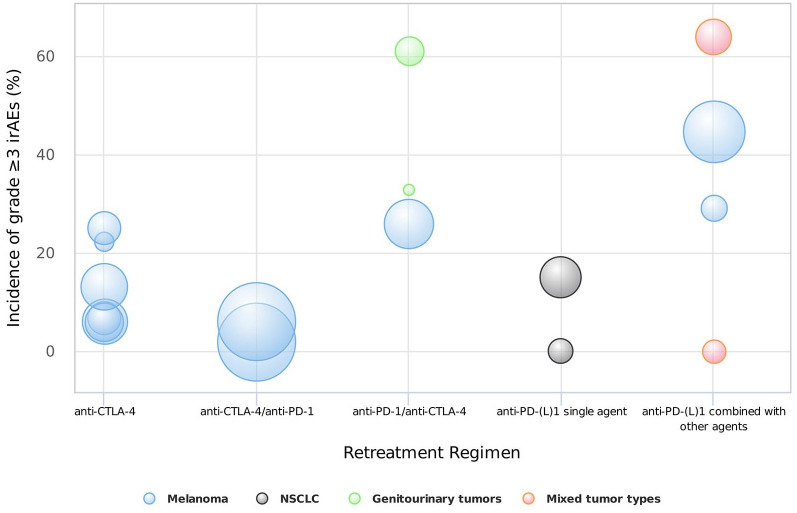
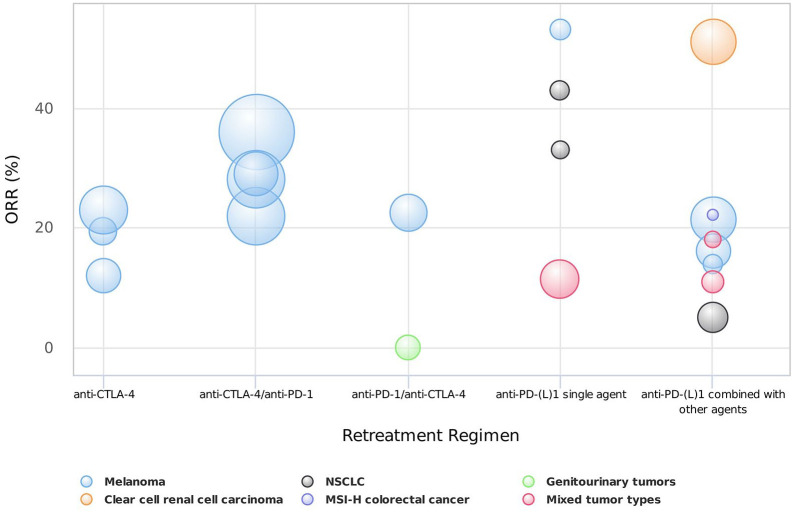
We identified 22 prospective studies including 1865 patients. For disease progression after CTLA-4 inhibitors, three studies evaluated anti-CTLA-4 retreatment. The ORR was 12-23%, the DCR was 48.4-67.7%, and the mOS was 12 months. The incidence of grade ⩾3 irAEs was 5.9-25%. Four studies evaluated anti-programmed cell death protein 1 (PD-1) retreatment. The ORR was 22-36%, the DCR was 40-64%, and the mOS was 13.4-20.6 months. The incidence of grade ⩾3 irAEs was <10%. For disease progression after PD-(L)1 inhibitors, 13 studies evaluated anti-PD-(L)1 retreatment. The ORR was 5-53%, the DCR was 38-83%, and the mOS was 13.9 months. The incidence of grade ⩾3 irAEs was 0-15% for patients retreated with single anti-PD-(L)1 agent, but was higher (0-64%) for those retreated with ICIs combined with other agents. Two studies evaluated anti-cytotoxic T-lymphocyte associated protein 4 (CTLA-4) retreatment. The ORR was 0-22.4%, the DCR was 50-72%, and the mOS was 4-21 months. The incidence of grade ⩾3 irAEs was 26-61%.
Retreatment with ICIs is feasible for cancer patients considering its encouraging efficacy and tolerable safety. Further prospective trials are needed to explore more promising strategies and identify suitable populations for retreatment.
尽管使用免疫检查点抑制剂(ICI)进行治疗,但仍有很大比例的患者最终会出现疾病进展,而该人群后续的治疗选择有限。使用相同或不同类型的ICI进行再治疗是一种可能的策略,但临床疗效和安全性数据有限。本系统评价旨在评估ICI再治疗对先前ICI治疗后疾病进展的实体瘤患者的疗效和安全性。
我们检索了MEDLINE、EMBASE、Cochrane图书馆和主要会议图书馆,以查找前瞻性研究。主要结局包括客观缓解率(ORR)、疾病控制率(DCR)、中位总生存期(mOS)以及≥3级免疫相关不良事件(irAE)的发生率。
我们纳入了22项前瞻性研究,共1865例患者。对于CTLA-4抑制剂治疗后疾病进展的情况,三项研究评估了抗CTLA-4再治疗。ORR为12%-23%,DCR为48.4%-67.7%,mOS为12个月。≥3级irAE的发生率为5.9%-25%。四项研究评估了抗程序性细胞死亡蛋白1(PD-1)再治疗。ORR为22%-36%,DCR为40%-64%,mOS为13.4-20.6个月。≥3级irAE的发生率<10%。对于PD-(L)1抑制剂治疗后疾病进展的情况,13项研究评估了抗PD-(L)1再治疗。ORR为5%-53%,DCR为38%-83%,mOS为13.9个月。接受单一抗PD-(L)1药物再治疗的患者≥3级irAE的发生率为0%-15%,但接受ICI与其他药物联合再治疗的患者发生率更高(0%-64%)。两项研究评估了抗细胞毒性T淋巴细胞相关蛋白4(CTLA-4)再治疗。ORR为0%-22.4%,DCR为50%-72%,mOS为4-21个月。≥3级irAE的发生率为26%-61%。
考虑到ICI再治疗令人鼓舞的疗效和可耐受的安全性,对癌症患者来说是可行的。需要进一步的前瞻性试验来探索更有前景的策略,并确定适合再治疗的人群。