VIP Department, Sun Yat-sen University Cancer Center, Guangzhou, China.
State Key Laboratory of Oncology in South China, Sun Yat-sen University Cancer Center, Guangzhou, China.
Front Immunol. 2022 Mar 2;13:801909. doi: 10.3389/fimmu.2022.801909. eCollection 2022.
Anti-programmed cell death protein 1 and its ligand (anti-PD1/PDL1) have been proposed as a promising therapeutic option for advanced biliary tract cancer (aBTC). Given the scarce quantitative analyses of anti-PD1/PDL1 in aBTC, we thus did a meta-analysis to assess the benefits and risks of this emerging treatment strategy in patients with aBTC.
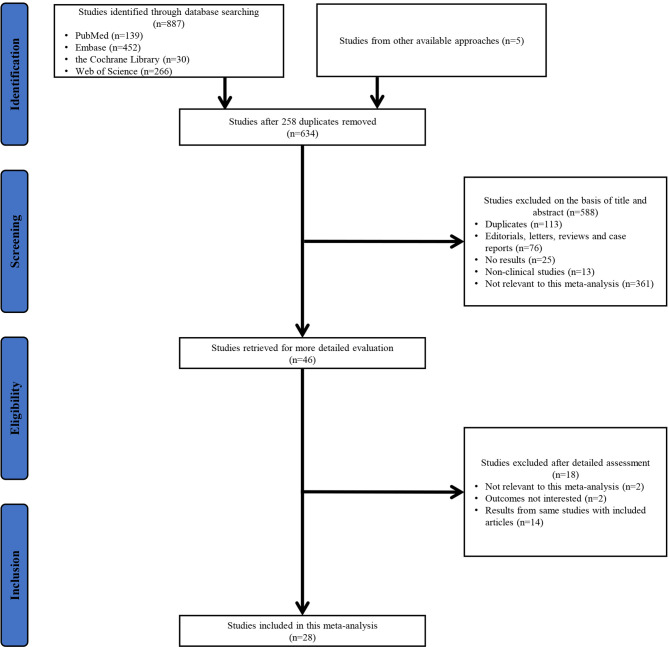
PubMed, Embase, the Cochrane Library, Web of Science, and meeting resources were searched for relevant studies. The main endpoints were median progression-free survival (mPFS), median overall survival (mOS), objective response rate (ORR), disease control rate (DCR), any-grade adverse events (AEs), and grade 3-4 AEs.
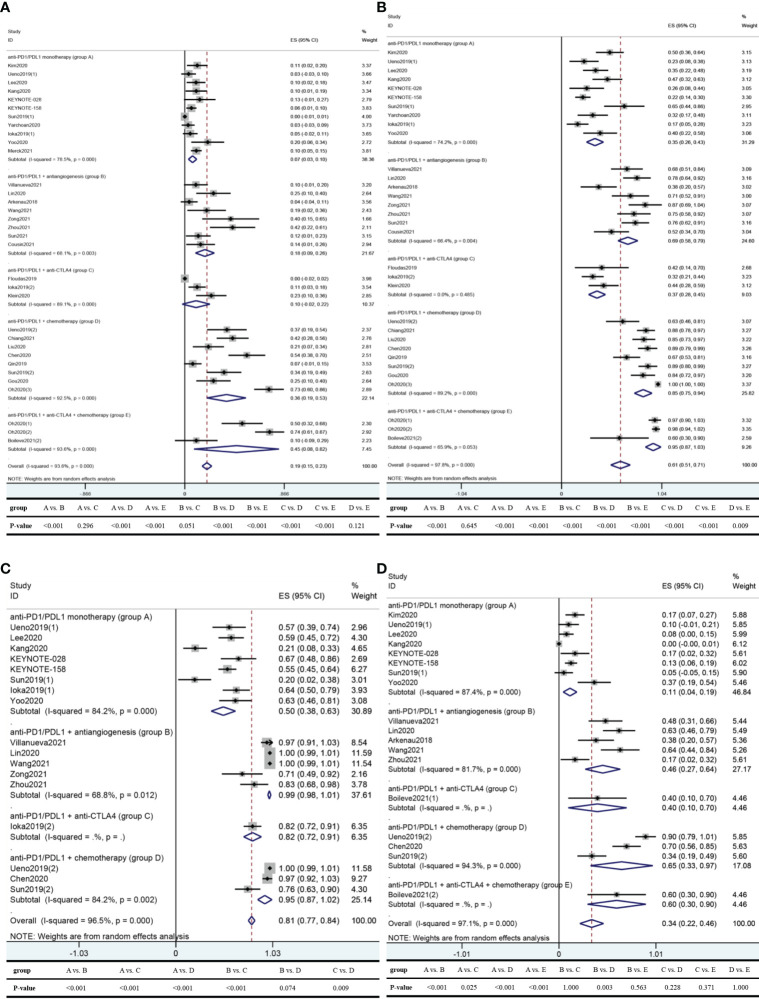
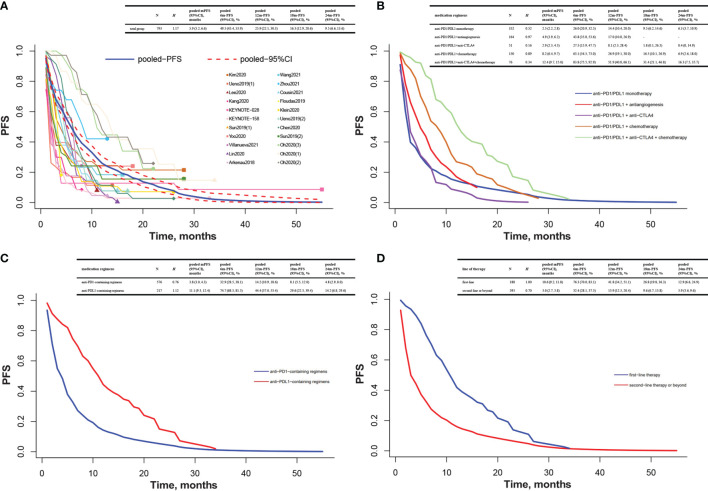
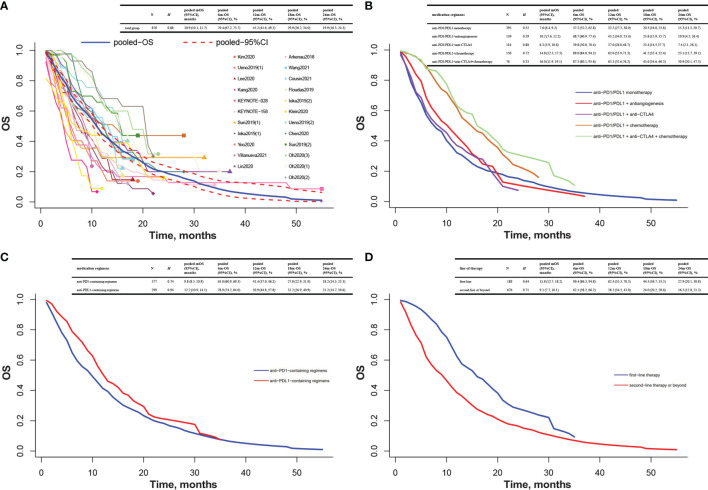
Twenty-eight studies with 1,338 participants were included. The best curative effect was found in the anti-PD1/PDL1 combined with anti-CTLA4 and chemotherapy group (mPFS: 12.4 months; mOS: 16.0 months; ORR: 45.1%; DCR: 95.0%), followed by the anti-PD1/PDL1 plus chemotherapy group (mPFS: 8.2 months; mOS: 14.8 months; ORR: 36.3%; DCR: 84.6%), the anti-PD1/PDL1 plus antiangiogenesis group (mPFS: 4.9 months; mOS: 10.2 months; ORR: 17.5%; DCR: 68.7%), the anti-PD1/PDL1 plus anti-cytotoxic T lymphocyte antigen 4 (anti-CTLA4) group (mPFS: 2.9 months; mOS: 8.3 months; ORR: 9.9%; DCR: 36.8%), and the anti-PD1/PDL1 monotherapy group (mPFS: 2.5 months; mOS: 7.6 months; ORR: 6.8%; DCR: 34.7%). Compared with anti-PD1-containing regimens, anti-PDL1-containing regimens achieved preferable mPFS (11.1 vs. 3.8 months), mOS (12.2 vs. 9.8 months), and ORR (23.7% vs. 17.4%), despite a similar DCR (61.1% vs. 61.3%). The mPFS, mOS, ORR, and DCR were 10.6 months, 15.8 months, 42.3%, and 88.6% of first-line anti-PD1/PDL1 and 3.0 months, 9.1 months, 11.6%, and 51.1% of second-line therapy or beyond, respectively. There were 80.6% and 34.0% of the patients suffering any-grade AEs and grade 3-4 AEs. Anti-PD1/PDL1 monotherapy might be considered as a safer alternative than combination regimens. Meanwhile, obvious toxicities in the first-line setting could not be neglected.
Anti-PD1/PDL1 showed encouraging efficacy and acceptable safety profile in aBTC and, thus, could be an alternative treatment.
抗程序性细胞死亡蛋白 1 及其配体(抗 PD1/PDL1)已被提出作为晚期胆道癌(aBTC)的一种有前途的治疗选择。鉴于对 aBTC 中抗 PD1/PDL1 的定量分析很少,因此我们进行了一项荟萃分析,以评估这种新兴治疗策略在 aBTC 患者中的获益和风险。
检索了 PubMed、Embase、Cochrane 图书馆、Web of Science 和会议资源中相关的研究。主要终点是中位无进展生存期(mPFS)、中位总生存期(mOS)、客观缓解率(ORR)、疾病控制率(DCR)、任何级别的不良事件(AE)和 3-4 级 AE。
纳入了 28 项研究,共计 1338 名参与者。最佳疗效见于抗 PD1/PDL1 联合抗 CTLA4 和化疗组(mPFS:12.4 个月;mOS:16.0 个月;ORR:45.1%;DCR:95.0%),其次是抗 PD1/PDL1 联合化疗组(mPFS:8.2 个月;mOS:14.8 个月;ORR:36.3%;DCR:84.6%)、抗 PD1/PDL1 联合抗血管生成组(mPFS:4.9 个月;mOS:10.2 个月;ORR:17.5%;DCR:68.7%)、抗 PD1/PDL1 联合抗细胞毒性 T 淋巴细胞抗原 4(抗 CTLA4)组(mPFS:2.9 个月;mOS:8.3 个月;ORR:9.9%;DCR:36.8%)和抗 PD1/PDL1 单药治疗组(mPFS:2.5 个月;mOS:7.6 个月;ORR:6.8%;DCR:34.7%)。与含抗 PD1 的方案相比,含抗 PDL1 的方案在 mPFS(11.1 与 3.8 个月)、mOS(12.2 与 9.8 个月)和 ORR(23.7%与 17.4%)方面具有更好的疗效,尽管 DCR 相似(61.1%与 61.3%)。一线抗 PD1/PDL1 的 mPFS、mOS、ORR 和 DCR 分别为 10.6 个月、15.8 个月、42.3%和 88.6%,二线或以上治疗的 mPFS、mOS、ORR 和 DCR 分别为 3.0 个月、9.1 个月、11.6%和 51.1%。分别有 80.6%和 34.0%的患者出现任何级别 AEs 和 3-4 级 AEs。抗 PD1/PDL1 单药治疗可能比联合治疗方案更安全。同时,一线治疗中明显的毒性作用不容忽视。
抗 PD1/PDL1 在 aBTC 中显示出令人鼓舞的疗效和可接受的安全性,因此可能是一种替代治疗方法。