Department of Clinical Sciences, Liverpool School of Tropical Medicine, Liverpool, UK.
Urgent Care, Team Medical, Paraparaumu, New Zealand.
Cochrane Database Syst Rev. 2020 Dec 8;12(12):CD003048. doi: 10.1002/14651858.CD003048.pub4.
Probiotics may be effective in reducing the duration of acute infectious diarrhoea.
To assess the effects of probiotics in proven or presumed acute infectious diarrhoea.
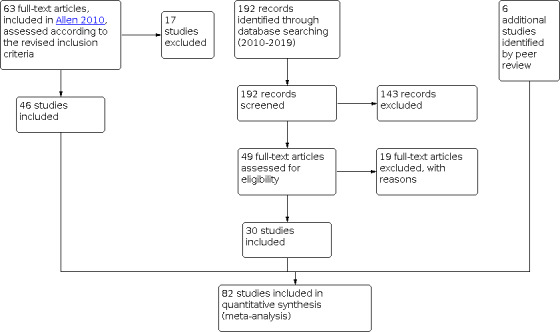
We searched the trials register of the Cochrane Infectious Diseases Group, MEDLINE, and Embase from inception to 17 December 2019, as well as the Cochrane Controlled Trials Register (Issue 12, 2019), in the Cochrane Library, and reference lists from studies and reviews. We included additional studies identified during external review.
Randomized controlled trials comparing a specified probiotic agent with a placebo or no probiotic in people with acute diarrhoea that is proven or presumed to be caused by an infectious agent.
Two review authors independently applied inclusion criteria, assessed risk of bias, and extracted data. Primary outcomes were measures of diarrhoea duration (diarrhoea lasting ≥ 48 hours; duration of diarrhoea). Secondary outcomes were number of people hospitalized in community studies, duration of hospitalization in inpatient studies, diarrhoea lasting ≥ 14 days, and adverse events.
We included 82 studies with a total of 12,127 participants. These studies included 11,526 children (age < 18 years) and 412 adults (three studies recruited 189 adults and children but did not specify numbers in each age group). No cluster-randomized trials were included. Studies varied in the definitions used for "acute diarrhoea" and "end of the diarrhoeal illness" and in the probiotic(s) tested. A total of 53 trials were undertaken in countries where both child and adult mortality was low or very low, and 26 where either child or adult mortality was high. Risk of bias was high or unclear in many studies, and there was marked statistical heterogeneity when findings for the primary outcomes were pooled in meta-analysis. Effect size was similar in the sensitivity analysis and marked heterogeneity persisted. Publication bias was demonstrated from funnel plots for the main outcomes. In our main analysis of the primary outcomes in studies at low risk for all indices of risk of bias, no difference was detected between probiotic and control groups for the risk of diarrhoea lasting ≥ 48 hours (risk ratio (RR) 1.00, 95% confidence interval (CI) 0.91 to 1.09; 2 trials, 1770 participants; moderate-certainty evidence); or for duration of diarrhoea (mean difference (MD) 8.64 hours shorter, 95% CI 29.4 hours shorter to 12.1 hours longer; 6 trials, 3058 participants; very low-certainty evidence). Effect size was similar and marked heterogeneity persisted in pre-specified subgroup analyses of the primary outcomes that included all studies. These included analyses limited to the probiotics Lactobacillus rhamnosus GG and Saccharomyces boulardii. In six trials (433 participants) of Lactobacillus reuteri, there was consistency amongst findings (I² = 0%), but risk of bias was present in all included studies. Heterogeneity also was not explained by types of participants (age, nutritional/socioeconomic status captured by mortality stratum, region of the world where studies were undertaken), diarrhoea in children caused by rotavirus, exposure to antibiotics, and the few studies of children who were also treated with zinc. In addition, there were no clear differences in effect size for the primary outcomes in post hoc analyses according to decade of publication of studies and whether or not trials had been registered. For other outcomes, the duration of hospitalization in inpatient studies on average was shorter in probiotic groups than in control groups but there was marked heterogeneity between studies (I² = 96%; MD -18.03 hours, 95% CI -27.28 to -8.78, random-effects model: 24 trials, 4056 participants). No differences were detected between probiotic and control groups in the number of people with diarrhoea lasting ≥ 14 days (RR 0.49, 95% CI 0.16 to 1.53; 9 studies, 2928 participants) or in risk of hospitalization in community studies (RR 1.26, 95% CI 0.84 to 1.89; 6 studies, 2283 participants). No serious adverse events were attributed to probiotics.
AUTHORS' CONCLUSIONS: Probiotics probably make little or no difference to the number of people who have diarrhoea lasting 48 hours or longer, and we are uncertain whether probiotics reduce the duration of diarrhoea. This analysis is based on large trials with low risk of bias.
益生菌可能对缩短急性感染性腹泻的持续时间有效。
评估益生菌对已证实或疑似急性感染性腹泻的疗效。
我们检索了 Cochrane 传染病组试验注册库、MEDLINE 和 Embase 数据库,检索日期截至 2019 年 12 月 17 日,同时检索了 Cochrane 图书馆中的 Cochrane 对照试验注册库(2019 年第 12 期)和综述中的参考文献列表。我们还在外部审查期间确定了其他研究。
比较特定益生菌与安慰剂或无益生菌治疗急性腹泻的随机对照试验,腹泻由感染性病原体引起已得到证实或疑似。
两名综述作者独立应用纳入标准、评估偏倚风险并提取数据。主要结局是腹泻持续时间(腹泻持续时间≥48 小时;腹泻持续时间)的测量指标。次要结局是社区研究中住院人数、住院研究中住院时间、腹泻持续时间≥14 天和不良事件。
我们纳入了 82 项研究,共计 12127 名参与者。这些研究包括 11526 名儿童(年龄<18 岁)和 412 名成年人(三项研究纳入了 189 名成年人和儿童,但未具体说明每个年龄组的人数)。没有纳入整群随机试验。研究在“急性腹泻”和“腹泻病结束”的定义以及测试的益生菌方面存在差异。其中 53 项研究在儿童和成人死亡率低或极低的国家进行,26 项研究在儿童或成人死亡率高的国家进行。许多研究的偏倚风险较高或不明确,并且当对主要结局进行荟萃分析时,结果存在显著的统计学异质性。敏感性分析中的效果大小相似,异质性仍然存在。漏斗图显示主要结局存在发表偏倚。在我们对所有偏倚风险指数低风险的研究进行的主要结局的主要分析中,益生菌组与对照组相比,腹泻持续时间≥48 小时的风险(风险比 1.00,95%置信区间 0.91 至 1.09;2 项试验,1770 名参与者;中等确定性证据)或腹泻持续时间(平均差值 8.64 小时更短,95%置信区间 29.4 小时更短至 12.1 小时更长;6 项试验,3058 名参与者;极低确定性证据)无差异。在包括所有研究的主要结局的预先指定亚组分析中,效果大小相似且存在显著的异质性。这些分析包括对 Lactobacillus rhamnosus GG 和 Saccharomyces boulardii 益生菌的分析。在 6 项(433 名参与者)Lactobacillus reuteri 的试验中,发现结果一致(I²=0%),但所有纳入的研究都存在偏倚风险。异质性也不能用参与者的类型(年龄、通过死亡率分层捕获的营养/社会经济地位、研究开展的世界区域)、轮状病毒引起的儿童腹泻、暴露于抗生素以及接受锌治疗的儿童的少数研究来解释。此外,根据研究发表的十年和试验是否注册,在事后分析中,主要结局的效果大小没有明显差异。在住院研究中,益生菌组的住院时间平均比对照组短,但研究之间存在显著的异质性(I²=96%;MD-18.03 小时,95%置信区间-27.28 至-8.78,随机效应模型:24 项试验,4056 名参与者)。在持续时间≥14 天的腹泻人数(RR 0.49,95%置信区间 0.16 至 1.53;9 项研究,2928 名参与者)或社区研究中的住院风险(RR 1.26,95%置信区间 0.84 至 1.89;6 项研究,2283 名参与者)方面,益生菌组与对照组无差异。没有严重的不良事件归因于益生菌。
益生菌可能对持续时间超过 48 小时的腹泻人数或腹泻持续时间没有明显影响,我们不确定益生菌是否能减少腹泻的持续时间。这一分析基于低偏倚风险的大型试验。