Department of Surgery, Heidelberg University Hospital, Im Neuenheimer Feld 420, 69120, Heidelberg, Germany.
Department of Gastroenterology, Heidelberg University Hospital, Im Neuenheimer Feld 410, 69120, Heidelberg, Germany.
BMC Surg. 2020 Dec 9;20(1):324. doi: 10.1186/s12893-020-00995-2.
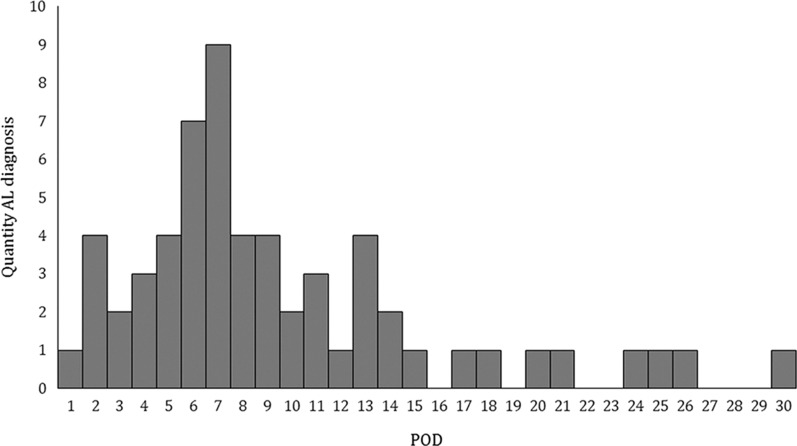
Early diagnosis of anastomotic leakage (AL) after esophageal resection is crucial for the successful management of this complication. Inflammatory serological markers are indicators of complications during the postoperative course. The aim of the present study was to evaluate the prognostic value of routine inflammatory markers to predict anastomotic leakage after transthoracic esophageal resection.
Data from all consecutive patients undergoing transthoracic esophageal resection between January 2010 and December 2016 were analyzed from a prospective database. Besides clinicodemographic parameters, C-reactive protein, white blood cell count and albumin were analyzed and the Noble/Underwood (NUn) score was calculated to evaluate their predictive value for postoperative anastomotic leakage. Diagnostic accuracy was measured by sensitivity, specificity, and negative and positive predictive values using area under the receiver operator characteristics curve.
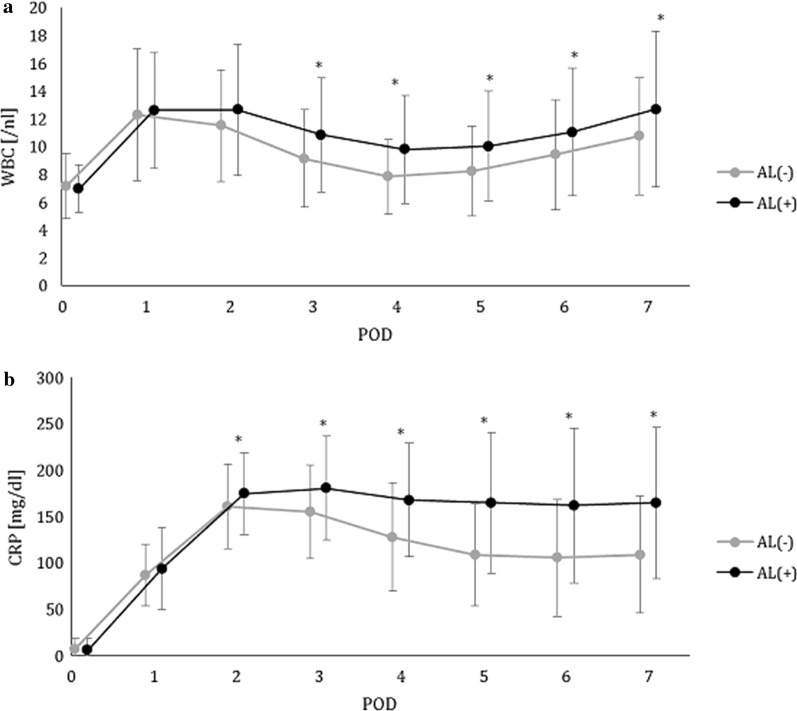
Overall, 233 patients with transthoracic esophageal resection were analyzed, 30-day mortality in this group was 3.4%. 57 patients (24.5%) suffered from AL, 176 patients were in the AL negative group. We found significant differences in WBCC, CRP and NUn scores between patients with and without AL, but the analyzed markers did not show an independent relevant prognostic value. For CRP levels below 155 mg/dl from POD3 to POD 7 the negative predictive value for absence of AI was > 80%. Highest diagnostic accuracy was detected for CRP levels on 4 POD with a cut-off value of 145 mg/l reaching negative predictive value of 87%.
In contrast to their prognostic value in other surgical procedures, CRP, WBCC and NUn score cannot be recommended as independent markers for the prediction of anastomotic leakage after transthoracic esophageal resection. CRP is an accurate negative predictive marker and discrimination of AL and no-AL may be helpful for postoperative clinical management. Trial registration The study was approved by the local ethical committee (S635-2013).
食管切除术后早期诊断吻合口漏(AL)对于成功处理这种并发症至关重要。炎症血清标志物是术后过程中并发症的指标。本研究旨在评估常规炎症标志物预测经胸食管切除术后吻合口漏的预后价值。
从一个前瞻性数据库中分析了 2010 年 1 月至 2016 年 12 月期间连续接受经胸食管切除术的所有患者的数据。除临床病理参数外,还分析了 C 反应蛋白、白细胞计数和白蛋白,并计算了 Noble/Underwood(NUn)评分,以评估其对术后吻合口漏的预测价值。使用接受者操作特征曲线下的面积来测量诊断准确性,包括敏感性、特异性、阴性和阳性预测值。
总体而言,分析了 233 例接受经胸食管切除术的患者,该组的 30 天死亡率为 3.4%。57 例(24.5%)患者发生 AL,176 例患者为 AL 阴性组。我们发现,有和无 AL 的患者之间的 WBCC、CRP 和 NUn 评分有显著差异,但分析的标志物没有显示出独立的相关预后价值。对于术后 3 至 7 天 CRP 水平低于 155mg/dl,无 AI 的阴性预测值>80%。在第 4 天 CRP 水平的检测中,诊断准确性最高,截断值为 145mg/L,阴性预测值为 87%。
与其他手术程序中的预后价值相比,CRP、WBCC 和 NUn 评分不能作为经胸食管切除术后吻合口漏预测的独立标志物。CRP 是一种准确的阴性预测标志物,区分 AL 和非 AL 可能有助于术后临床管理。
该研究得到了当地伦理委员会的批准(S635-2013)。