Bradshaw Pamela J, Tohira Hideo, Marangou James, Newman Mark, Reményi Bo, Wade Vicki, Reid Christopher, Katzenellenbogen Judith M
The School of Population and Global Health, The University of Western Australia, Australia.
Fiona Stanley Hospital, 11 Robin Warren Drive Murdoch, WA, 6150, Australia.
Ann Med Surg (Lond). 2020 Nov 25;60:557-565. doi: 10.1016/j.amsu.2020.11.055. eCollection 2020 Dec.
Australia, although a high income economy, carries a significant burden of rheumatic heart disease (RHD). Acute rheumatic fever (ARF) and RHD are endemic in the Indigenous population. Immigrants from low/lower-income countries ('non-Indigenous high-risk') are also at increased risk compared with 'non-Indigenous low-risk' Australians. This study describes the utilisation of surgical and percutaneous procedures for RHD-related valve disease among patients aged less than 50 years, from 2002 to 2017.
A descriptive study using data from the 'End RHD in Australia: Study of Epidemiology (ERASE) Project' linking RHD Registers and hospital inpatient data from five states/territories, and two surgical databases. Trends across three-year periods were determined and post-procedural all-cause 30-day mortality calculated.
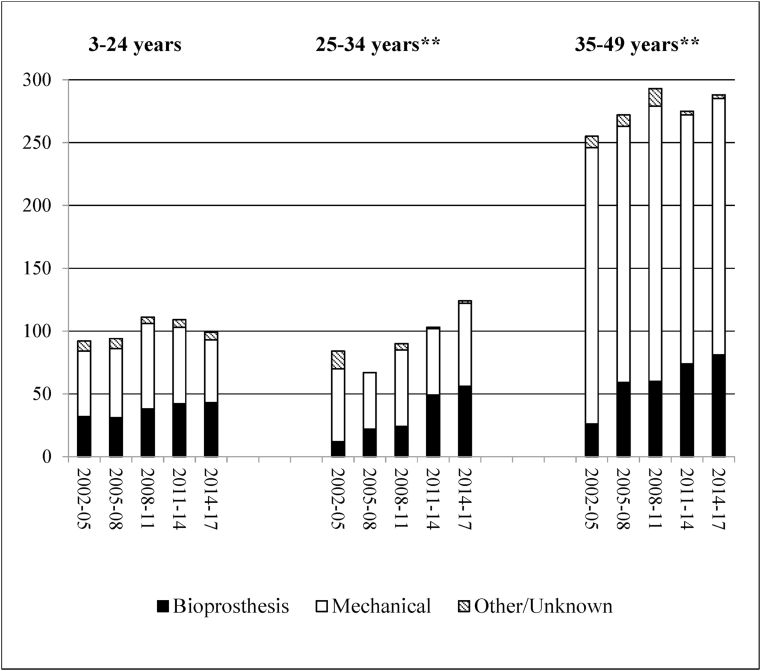
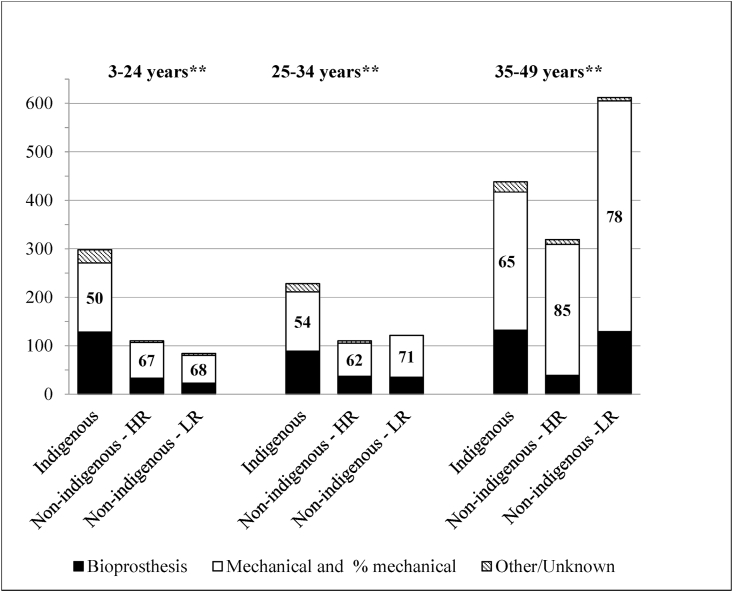
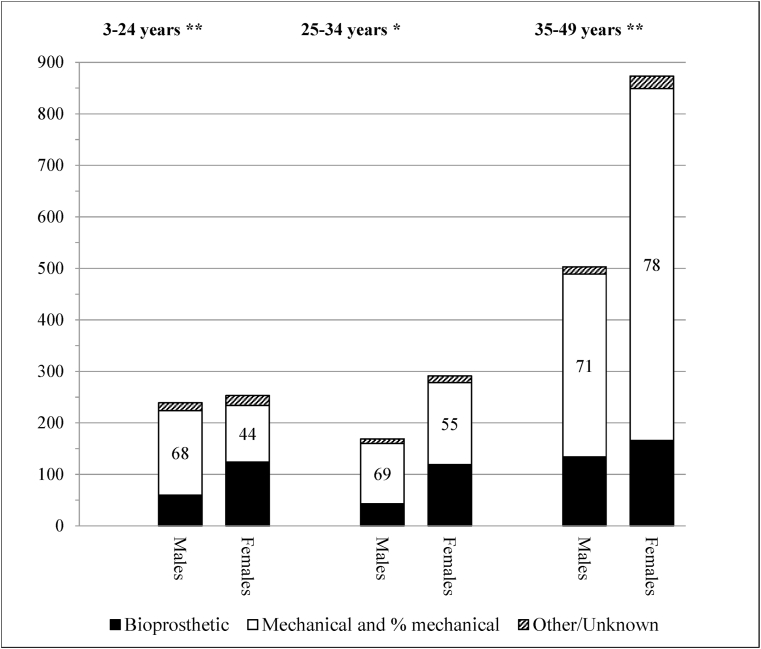
A total of 3900 valves interventions were undertaken in 3028 procedural episodes among 2487 patients. Over 50% of patients were in the 35-49 years group, and 64% were female. Over 60% of procedures for 3-24 year-olds were for Indigenous patients. There were few significant changes across the study period other than downward trends in the number and proportion of procedures for young Indigenous patients (3-24 years) and 'non-Indigenous/low risk' patients aged ≥35 years. Mitral valve procedures predominated, and multi-valve interventions increased, including on the tricuspid valve. The majority of replacement prostheses were mechanical, although bioprosthetic valve use increased overall, being highest among females <35 years and Indigenous Australians. All-cause mortality (n = 42) at 30-days was 1.4% overall (range 1.1-1.7), but 2.0% for Indigenous patients.
The frequency of cardiac valve procedures, and 30-day mortality remained steady across 15 years. Some changes in the distribution of procedures in population groups were evident. Replacement procedures, the use of bioprosthetic valves, and multiple-valve interventions increased. The challenge for Australian public health officials is to reduce the incidence, and improve the early detection and management of ARF/RHD in high-risk populations within Australia.
澳大利亚虽是高收入经济体,但风湿性心脏病(RHD)负担沉重。急性风湿热(ARF)和RHD在原住民中呈地方流行。与“非原住民低风险”澳大利亚人相比,来自低收入/中低收入国家的移民(“非原住民高风险”)患病风险也更高。本研究描述了2002年至2017年间50岁以下RHD相关瓣膜病患者手术和经皮手术的使用情况。
一项描述性研究,使用来自“澳大利亚终结RHD:流行病学研究(ERASE)项目”的数据,该项目将RHD登记册与五个州/领地的医院住院数据以及两个手术数据库相链接。确定三年期间的趋势,并计算术后30天全因死亡率。
2487例患者的3028次手术中,共进行了3900次瓣膜干预。超过50%的患者年龄在35 - 49岁组,64%为女性。3至24岁患者中超过60%的手术是针对原住民患者。除了年轻原住民患者(3至24岁)和≥35岁的“非原住民/低风险”患者手术数量和比例呈下降趋势外,研究期间几乎没有显著变化。二尖瓣手术占主导,多瓣膜干预增加,包括三尖瓣手术。大多数置换假体是机械瓣膜,尽管生物瓣膜的使用总体上有所增加,在35岁以下女性和澳大利亚原住民中最高。30天全因死亡率(n = 42)总体为1.4%(范围1.1 - 1.7),但原住民患者为2.0%。
心脏瓣膜手术的频率和30天死亡率在15年中保持稳定。人群组手术分布有一些明显变化。置换手术、生物瓣膜的使用和多瓣膜干预增加。澳大利亚公共卫生官员面临的挑战是降低发病率,并改善澳大利亚高危人群中ARF/RHD的早期检测和管理。