Wang Weidong, Xia Pinghui, Pan Liang, Xu Jinming, Lv Wang, Hu Jian
Department of Thoracic Surgery, The First Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, China.
Front Surg. 2020 Nov 9;7:584578. doi: 10.3389/fsurg.2020.584578. eCollection 2020.
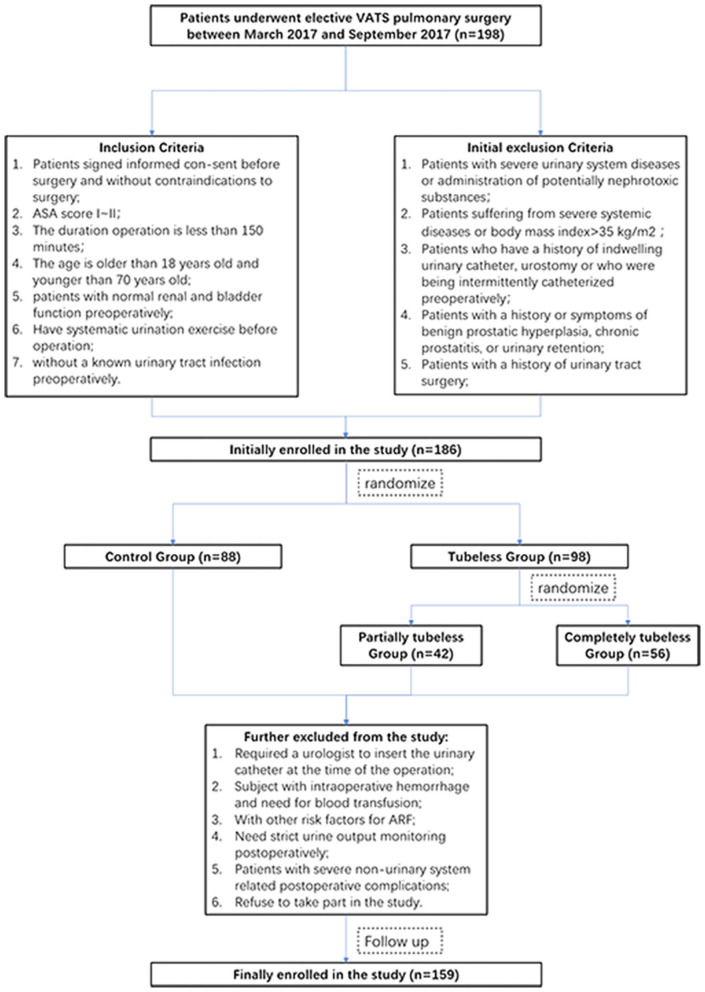
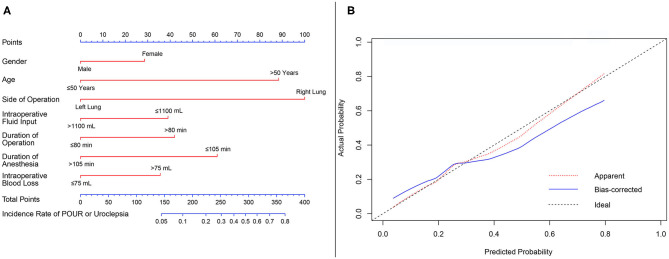
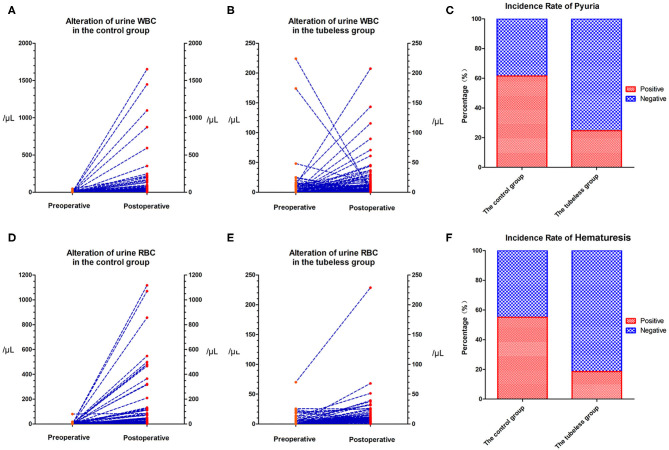
Although previous studies have shown the feasibility of non-intubated techniques, it is unknown whether avoiding urinary catheters can enhance recovery. This study aimed to determine whether the tubeless urinary catheter protocol is feasible and beneficial for minimally invasive lung surgery. Patients were randomized to the control group, completely tubeless group, and partially tubeless group. A propensity score-matched (PSM) analysis was performed to balance the non-random baseline characteristics. Complications and postoperative recovery were compared. Regression analysis was performed to identify the independent predictors of complications. A nomogram for predicting the risk of non-automatic micturition was constructed and internally validated. One hundred fifty-nine patients were enrolled. The incidence rates of urinary irritation and urinary tract infection (UTI) were significantly lower in the tubeless groups (74.4 vs. 39.5%, < 0.001; 28.2 vs. 8.6%, = 0.001, respectively). The tubeless group had a higher proportion of 0-degree discomfort (81.5 vs. 30.8%, = 0.001) and shorter duration of postoperative hospital stay than the control group (4.59 vs. 5.53 days, < 0.001). No difference was observed in terms of urination retention and urinary incontinence between the tubeless group and the control group. After PSM, the advantages of the tubeless group still existed, and comparing to the partially tubeless group, the completely tubeless group was of even less UTI and more 0-degree discomfort (18.5 vs. 0.0%, = 0.019; 96.3 vs. 59.3%, = 0.002). The tubeless protocol was the only independent protective factor of urinary complications. A nomogram was constructed and showed good predictive ability. The tubeless catheterization protocol led to fewer complications, better compliance, and shorter hospital length of stay. The advantages were more significant with the completely tubeless protocol. The utility of our nomogram can assist clinicians in avoiding risks in performing the tubeless protocol.
尽管先前的研究已表明非插管技术的可行性,但尚不清楚避免使用导尿管是否能促进恢复。本研究旨在确定无管导尿方案对微创肺手术是否可行且有益。患者被随机分为对照组、完全无管组和部分无管组。进行倾向评分匹配(PSM)分析以平衡非随机的基线特征。比较并发症和术后恢复情况。进行回归分析以确定并发症的独立预测因素。构建了预测非自主性排尿风险的列线图并进行了内部验证。共纳入159例患者。无管组的尿道刺激和尿路感染(UTI)发生率显著更低(分别为74.4%对39.5%,<0.001;28.2%对8.6%,=0.001)。与对照组相比,无管组0度不适的比例更高(81.5%对30.8%,=0.001),术后住院时间更短(4.59天对5.53天,<0.001)。无管组和对照组在排尿潴留和尿失禁方面未观察到差异。PSM后,无管组的优势仍然存在,与部分无管组相比,完全无管组的UTI更少,0度不适更多(18.5%对0.0%,=0.019;96.3%对59.3%,=0.002)。无管方案是尿路并发症的唯一独立保护因素。构建的列线图显示出良好的预测能力。无管导尿方案导致的并发症更少、依从性更好且住院时间更短。完全无管方案的优势更为显著。我们列线图的实用性可帮助临床医生在实施无管方案时避免风险。