Department of Hepatology and Gastroenterology, Niguarda Hospital, Milan, Italy.
Department of General and Digestive Surgery, Hospital Clínic, Institut d'Investigacion Biomediques August Pi-Sunyer (IDIBAPS) Centro de Investigación Biomédica en Red de Enfermedades Hepáticas y Digestivas (CIBERehd), University of Barcelona, Barcelona, Spain.
Gastroenterology. 2021 Mar;160(4):1151-1163.e3. doi: 10.1053/j.gastro.2020.11.045. Epub 2020 Dec 9.
Despite concerns that liver transplant (LT) recipients may be at increased risk of unfavorable outcomes from COVID-19 due the high prevalence of co-morbidities, immunosuppression and ageing, a detailed analysis of their effects in large studies is lacking.
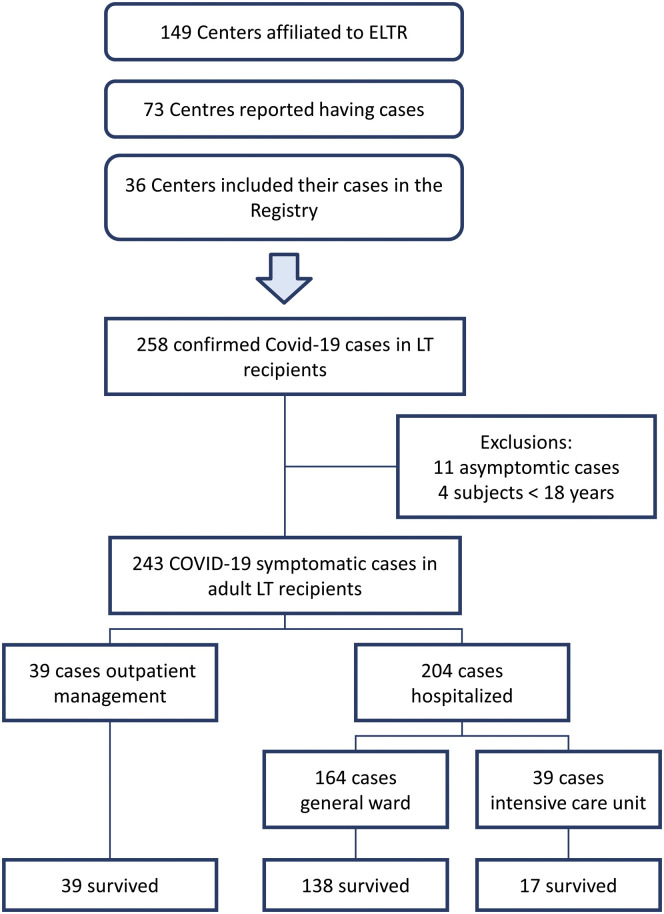
Data from adult LT recipients with laboratory confirmed SARS-CoV2 infection were collected across Europe. All consecutive patients with symptoms were included in the analysis.
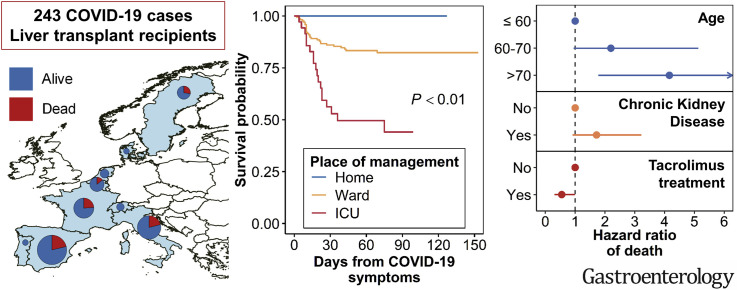
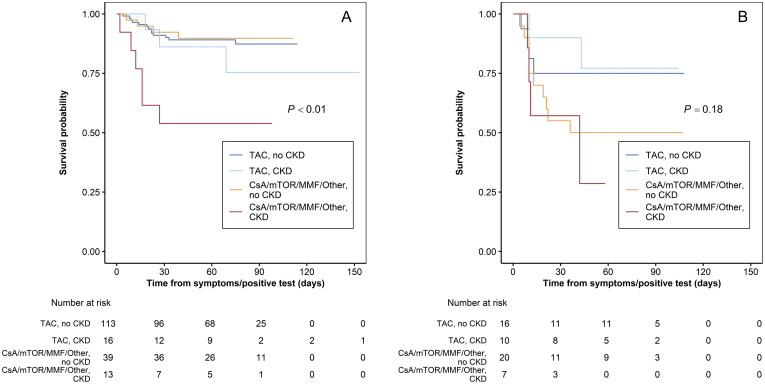
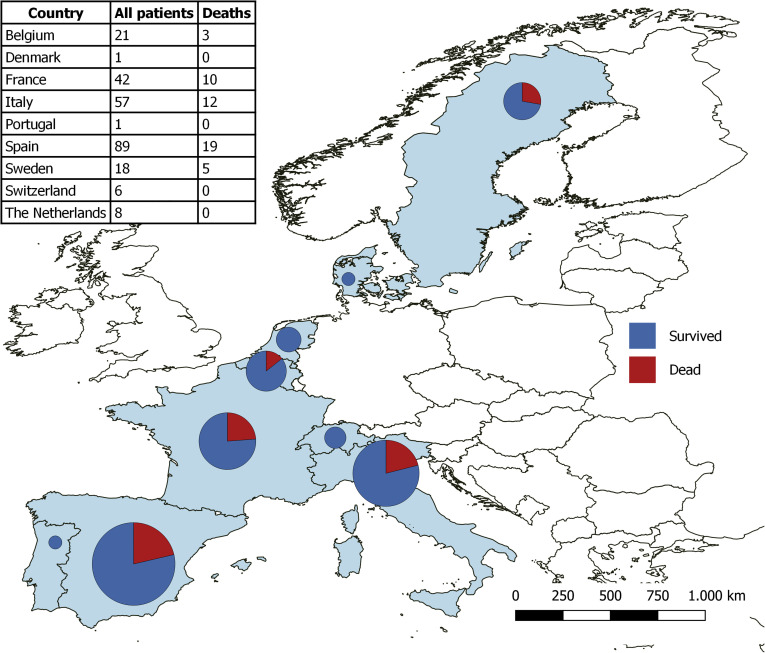
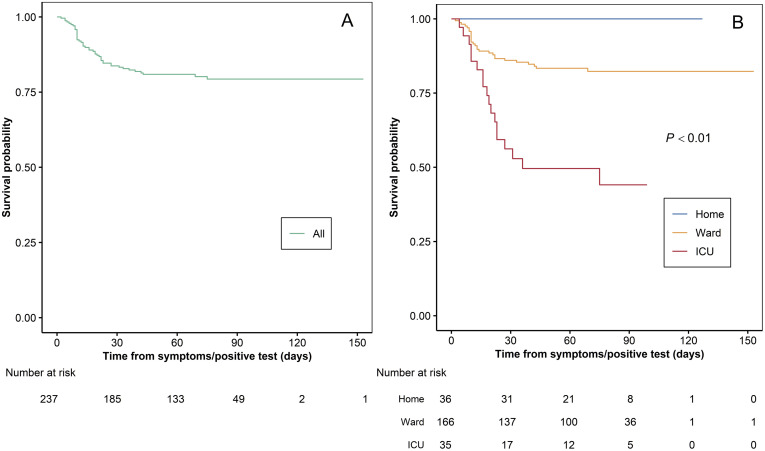
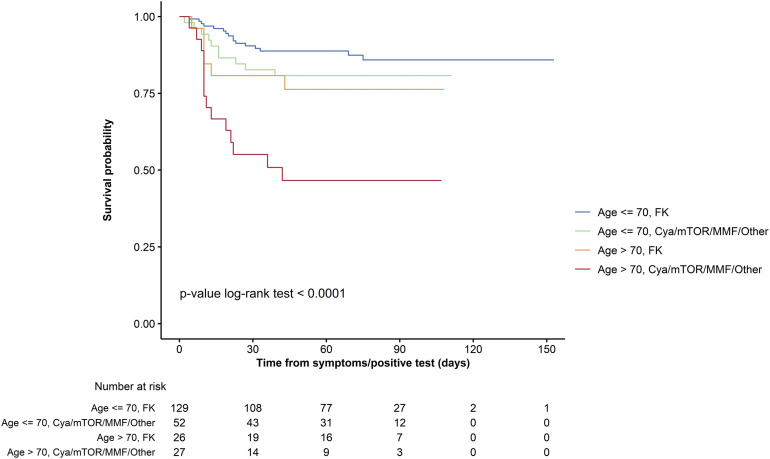
Between March 1 and June 27, 2020, data from 243 adult symptomatic cases from 36 centers and 9 countries were collected. Thirty-nine (16%) were managed as outpatients while 204 (84%) required hospitalization including admission to the ICU (39 of 204, 19.1%). Forty-nine (20.2%) patients died after a median of 13.5 (10-23) days, respiratory failure was the major cause. After multivariable Cox regression analysis, age >70 (HR, 4.16; 95% CI, 1.78-9.73) had a negative effect and tacrolimus (TAC) use (HR, 0.55; 95% CI, 0.31-0.99) had a positive independent effect on survival. The role of co-morbidities was strongly influenced by the dominant effect of age where comorbidities increased with the increasing age of the recipients. In a second model excluding age, both diabetes (HR, 1.95; 95% CI, 1.06-3.58) and chronic kidney disease (HR, 1.97; 95% CI, 1.05-3.67) emerged as associated with death CONCLUSIONS: Twenty-five percent of patients requiring hospitalization for COVID-19 died, the risk being higher in patients older than 70 and with medical co-morbidities, such as impaired renal function and diabetes. Conversely, the use of TAC was associated with a better survival thus encouraging clinicians to keep TAC at the usual dose.
尽管由于合并症、免疫抑制和老龄化的高发,肝移植(LT)受者因 COVID-19 而出现不良结局的风险可能增加,但在大型研究中缺乏对其影响的详细分析。
从欧洲各地收集了实验室确诊 SARS-CoV2 感染的成年 LT 受者的数据。所有出现症状的连续患者均纳入分析。
2020 年 3 月 1 日至 6 月 27 日,从 9 个国家的 36 个中心收集了 243 例有症状的成年病例数据。39 例(16%)作为门诊患者进行管理,而 204 例(84%)需要住院治疗,包括入住 ICU(204 例中有 39 例,19.1%)。49 例(20.2%)患者在中位 13.5(10-23)天后死亡,呼吸衰竭是主要原因。多变量 Cox 回归分析后,年龄>70 岁(HR,4.16;95%CI,1.78-9.73)对生存有负面影响,而他克莫司(TAC)的使用(HR,0.55;95%CI,0.31-0.99)对生存有积极的独立影响。合并症的作用受到受者年龄的主导作用的强烈影响,随着受者年龄的增加,合并症也随之增加。在排除年龄的第二个模型中,糖尿病(HR,1.95;95%CI,1.06-3.58)和慢性肾脏病(HR,1.97;95%CI,1.05-3.67)均与死亡相关。
需要住院治疗 COVID-19 的患者中有 25%死亡,年龄>70 岁且有肾功能不全和糖尿病等合并症的患者风险更高。相反,TAC 的使用与更好的生存相关,因此鼓励临床医生保持 TAC 的常规剂量。