Tokyo Bay Urayasu Ichikawa Medical Center, Chiba, Japan.
Department of Internal Medicine, Tokyo Dental College, Chiyoda City, Japan.
Hypertens Res. 2021 May;44(5):508-517. doi: 10.1038/s41440-020-00590-1. Epub 2020 Dec 14.
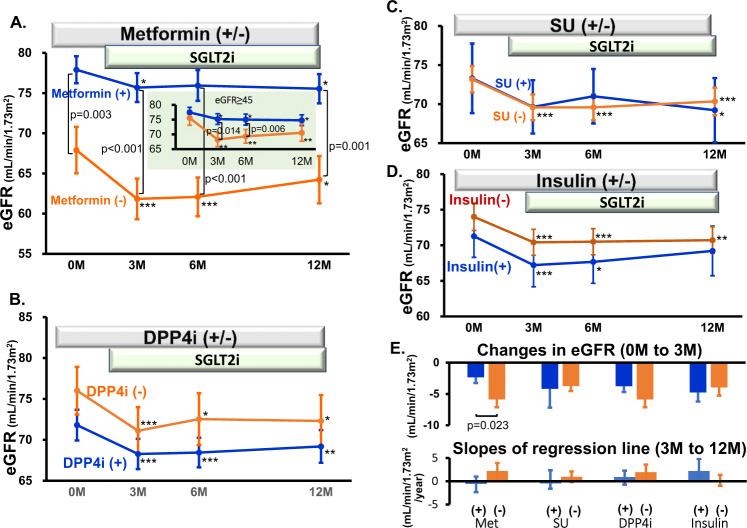
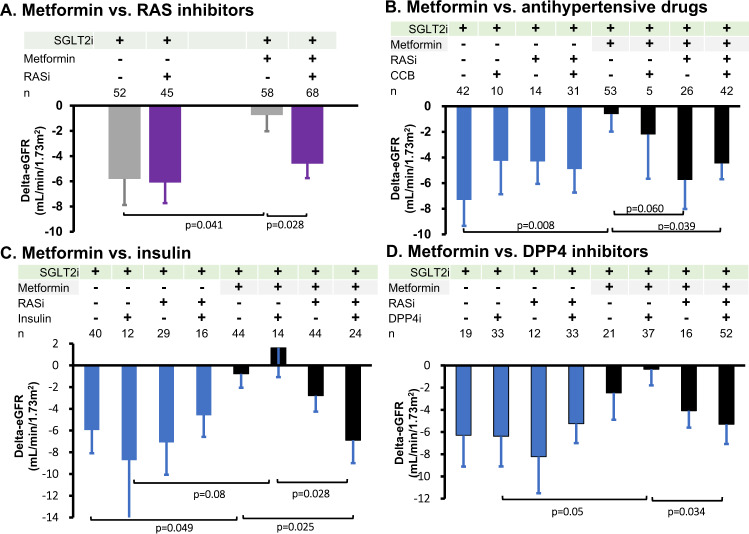
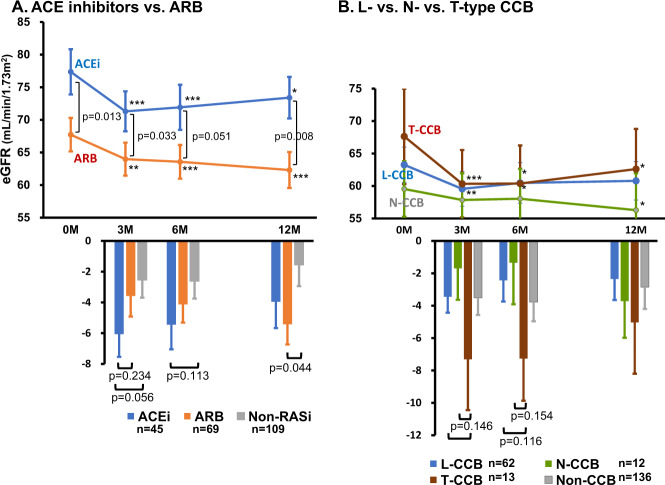
Recent randomized trials demonstrating the beneficial effects of sodium-glucose cotransporter 2 inhibitors (SGLT2is) in type 2 diabetes suggest that early reductions in eGFR upon initiation of SGLT2i therapy are associated with improved renal outcomes. Multiple concomitant medications, including antidiabetic and antihypertensive agents, are commonly used, however, which may modify the renal hemodynamic action of SGLT2is. Here we found that background treatment with metformin diminished the SGLT2i-induced reductions in eGFR after 3 months of SGLT2i therapy in patients with type 2 diabetes and hypertension (-2.29 ± 0.90 vs -5.85 ± 1.27 mL/min/1.73 m for metformin users (n = 126) and nonusers (n = 97), respectively). Other antidiabetic agents (DPP4 inhibitors, sulfonylureas and insulin) had no effect on the eGFR response to SGLT2is. Antihypertensive drugs, including calcium channel blockers (CCBs) and β blockers, did not affect the SGLT2i-induced changes in eGFR, whereas renin-angiotensin system inhibitors (RASis) tended to enhance this response (p = 0.059). Next, we evaluated the interaction between metformin and RASis in the eGFR responses to SGLT2is. Under no background treatment with RASis, metformin abrogated the eGFR response to SGLT2is, but this response was preserved when RASis had been given along with metformin (decreases of 0.75 ± 1.28 vs. 4.60 ± 1.15 mL/min/1.73 m in eGFR, p = 0.028). No interaction between metformin and insulin or between metformin and DPP4 inhibitors was observed. In conclusion, metformin blunts the SGLT2i-induced decrease in eGFR, but coadministration of RASis ameliorates this response. Furthermore, the inability of CCBs to modify the SGLT2i-induced reduction in eGFR suggests that the SGLT2i-induced renal microvascular action is mediated predominantly by postglomerular vasodilation rather than preglomerular vasoconstriction.
最近的随机临床试验表明,钠-葡萄糖共转运蛋白 2 抑制剂(SGLT2i)对 2 型糖尿病的有益作用表明,SGLT2i 治疗开始时 eGFR 的早期降低与改善肾脏结局相关。然而,经常同时使用多种合并药物,包括抗糖尿病和抗高血压药物,这些药物可能会改变 SGLT2i 的肾脏血流动力学作用。在这里,我们发现,在患有 2 型糖尿病和高血压的患者中,在接受 SGLT2i 治疗 3 个月后,背景治疗中的二甲双胍会减弱 SGLT2i 引起的 eGFR 降低(分别为二甲双胍使用者(n=126)和非使用者(n=97)的-2.29±0.90 与-5.85±1.27 mL/min/1.73 m)。其他抗糖尿病药物(DPP4 抑制剂、磺酰脲类药物和胰岛素)对 SGLT2i 引起的 eGFR 反应没有影响。降压药物,包括钙通道阻滞剂(CCBs)和β受体阻滞剂,不会影响 SGLT2i 引起的 eGFR 变化,而肾素-血管紧张素系统抑制剂(RASi)则倾向于增强这种反应(p=0.059)。接下来,我们评估了二甲双胍和 RASi 在 SGLT2i 对 eGFR 反应中的相互作用。在没有 RASi 背景治疗的情况下,二甲双胍阻断了 SGLT2i 对 eGFR 的反应,但当 RASi 与二甲双胍一起给予时,这种反应得到了保留(eGFR 的降低分别为 0.75±1.28 与 4.60±1.15 mL/min/1.73 m,p=0.028)。未观察到二甲双胍与胰岛素或二甲双胍与 DPP4 抑制剂之间的相互作用。总之,二甲双胍会削弱 SGLT2i 引起的 eGFR 降低,但 RASi 的联合给药可改善这种反应。此外,CCBs 无法改变 SGLT2i 引起的 eGFR 降低表明,SGLT2i 引起的肾脏微血管作用主要是通过肾小球后血管扩张而不是肾小球前血管收缩介导的。