Department of Emergency Medicine, Stanford University, Stanford, California.
Stanford University School of Medicine, Stanford, California.
JAMA Netw Open. 2020 Dec 1;3(12):e2025860. doi: 10.1001/jamanetworkopen.2020.25860.
The US Government Accountability Office has changed its estimate of the annual costs of defensive medicine, largely because it has been difficult to objectively measure its impact. Evaluating the association of malpractice claims rates with hospital admission rates and the costs of admitting patients with low-risk conditions would help to document the impact of defensive medicine. Although syncope is a concerning symptom, most patients with syncope have a low risk of adverse outcomes. However, many low-risk patients are still admitted to the hospital, with associated costs of more than $2.5 billion per year in the US.
To assess whether hospital admission rates after emergency department visits among patients with lower-risk syncope are associated with state-level variations in malpractice claims rates.
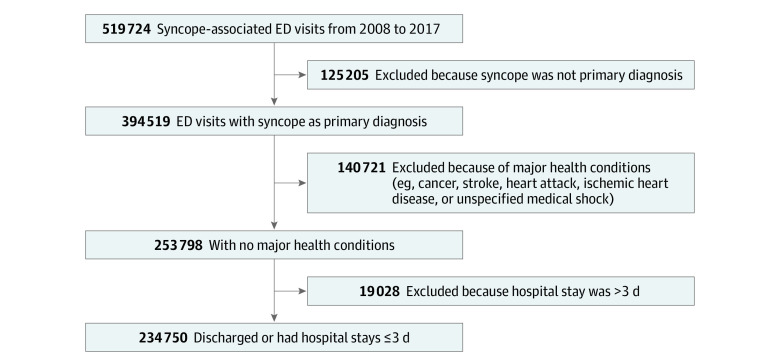
DESIGN, SETTING, AND PARTICIPANTS: This cross-sectional study of emergency department visits among patients with lower-risk syncope used deidentified data from the Clinformatics Data Mart database (Optum). Lower-risk syncope visits were defined as those with a primary diagnosis of syncope and collapse based on International Classification of Diseases, Ninth Revision, Clinical Modification code 780.2 or International Classification of Diseases, Tenth Revision, Clinical Modification code R55 that did not include another major diagnostic code for a condition requiring hospital admission (such as heart disease, cancer, or medical shock) or an inpatient hospital stay of more than 3 days. These data were linked to publicly available data from the National Practitioner Data Bank pertaining to physician malpractice claims between January 1, 2008, and December 31, 2017. The 2 data sets were linked at the state-year level. Data were analyzed from October 2, 2019, to September 12, 2020.
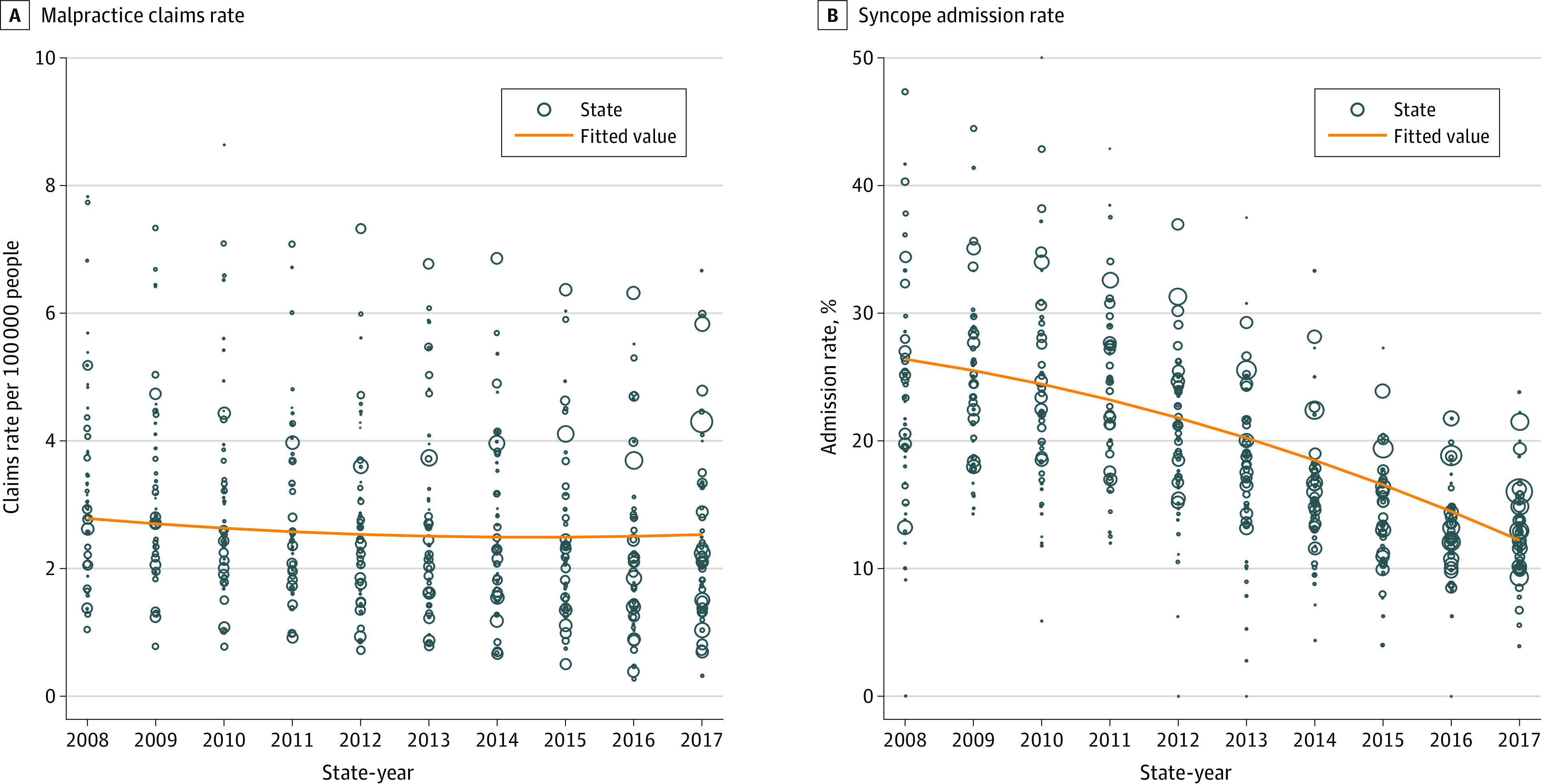
The association between the rate of hospital admission after emergency department visits among patients with lower-risk syncope and the rate of physician malpractice claims was assessed at the state-year level using a state-level fixed-effects model. Standardized costs obtained from the Clinformatics Data Mart database were adjusted for inflation and expressed in 2017 US dollars using the Consumer Price Index.
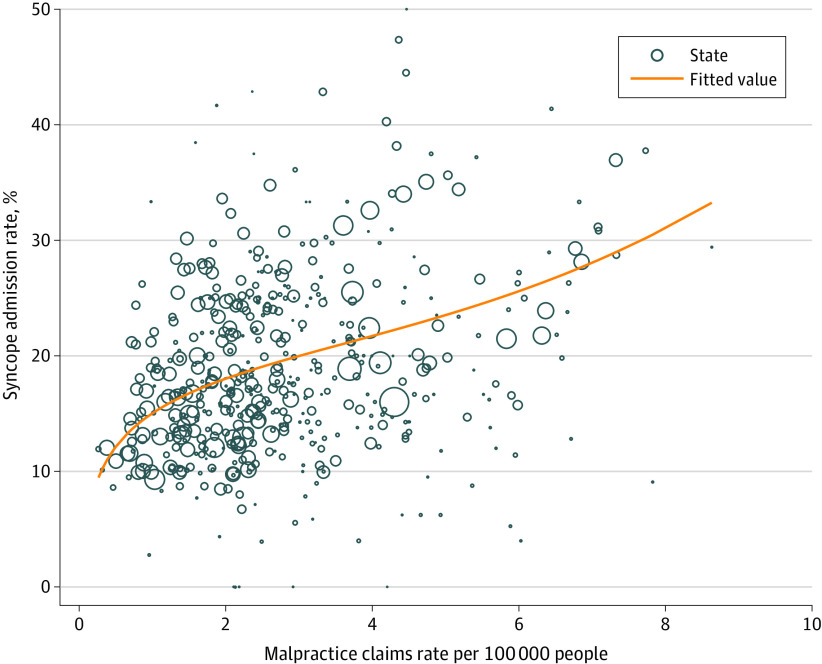
Among 40 482 813 emergency department visits between 2008 and 2017, 519 724 visits (1.3%) were associated with syncope. Of those, 234 750 visits (45.2%) met the criteria for lower-risk syncope. The mean (SD) age of patients in the lower-risk cohort was 71.8 (13.5) years; 141 050 patients (60.1%) were female, and 44 115 patients (18.8%) were admitted to the hospital, representing an extra cost of $6542 per admission. The mean rate of physician malpractice claims varied from 0.27 claims per 100 000 people to 8.63 claims per 100 000 people across states and across years within states. A state-level fixed-effects regression model indicated that, for every 1 in 100 000-person increase in the physician malpractice claims rate, there was an absolute increase of 6.70% (95% CI, 4.65%-8.75%) or a relative increase of 35.6% in the hospital admission rate, which represented an additional $102 million in costs associated with this lower-risk cohort.
In this study, increases in physician malpractice claims rates were associated with increases in hospital admission rates and substantial health care costs for patients with lower-risk syncope, and these increases are likely associated with the practice of defensive medicine.
美国政府问责局已经改变了对防御性医疗年度成本的估计,主要是因为很难客观衡量其影响。评估医疗事故索赔率与医院入院率以及低风险患者入院成本之间的关联将有助于记录防御性医疗的影响。虽然晕厥是一种令人担忧的症状,但大多数晕厥患者的不良预后风险较低。然而,许多低风险患者仍被收入医院,在美国每年的相关费用超过 25 亿美元。
评估急诊就诊的低风险晕厥患者的入院率是否与州级别的医疗事故索赔率有关。
设计、设置和参与者:本研究使用 Optum 的 Clinformatics Data Mart 数据库中的匿名数据,对低风险晕厥的急诊就诊患者进行了横断面研究。低风险晕厥就诊的定义是,基于国际疾病分类,第九修订版临床修正(International Classification of Diseases, Ninth Revision, Clinical Modification)代码 780.2 或国际疾病分类,第十修订版临床修正(International Classification of Diseases, Tenth Revision, Clinical Modification)代码 R55,主要诊断为晕厥和跌倒,不包括需要住院治疗的其他主要诊断代码(如心脏病、癌症或医学性休克)或住院时间超过 3 天。这些数据与 2008 年 1 月 1 日至 2017 年 12 月 31 日期间全国执业医师数据银行公开提供的医生医疗事故索赔数据相关联。两个数据集在州-年水平上进行了链接。数据分析于 2019 年 10 月 2 日至 2020 年 9 月 12 日进行。
在州-年水平上,使用州级固定效应模型评估低风险晕厥患者急诊就诊后住院率与医生医疗事故索赔率之间的关联。从 Clinformatics Data Mart 数据库获得的标准化成本按通胀进行了调整,并使用消费者价格指数(Consumer Price Index)以 2017 年美元表示。
在 2008 年至 2017 年期间的 40482813 次急诊就诊中,519724 次(1.3%)与晕厥有关。其中,234750 次(45.2%)符合低风险晕厥的标准。低风险队列患者的平均(标准差)年龄为 71.8(13.5)岁;141050 名患者(60.1%)为女性,44115 名患者(18.8%)入院,每次入院的额外费用为 6542 美元。医生医疗事故索赔的平均发生率在各州之间从每 10 万人中有 0.27 项索赔到每 10 万人中有 8.63 项索赔不等,在各州内的每年也有变化。州级固定效应回归模型表明,每增加 10 万人中有 1 项医生医疗事故索赔,医院入院率就会绝对增加 6.70%(95%CI,4.65%-8.75%)或相对增加 35.6%,这意味着与该低风险队列相关的额外费用增加了 1.02 亿美元。
在这项研究中,医生医疗事故索赔率的上升与低风险晕厥患者的入院率上升和大量医疗保健费用有关,这些上升很可能与防御性医疗实践有关。