St. Anna Children's Hospital, Children's Cancer Research Institute, University Vienna, Vienna, Austria.
Hôpital Robert Debré, GH APHP-Nord Université de Paris, Paris, France.
J Clin Oncol. 2021 Feb 1;39(4):295-307. doi: 10.1200/JCO.20.02529. Epub 2020 Dec 17.
Total body irradiation (TBI) before allogeneic hematopoietic stem cell transplantation (HSCT) in pediatric patients with acute lymphoblastic leukemia (ALL) is efficacious, but long-term side effects are concerning. We investigated whether preparative combination chemotherapy could replace TBI in such patients.
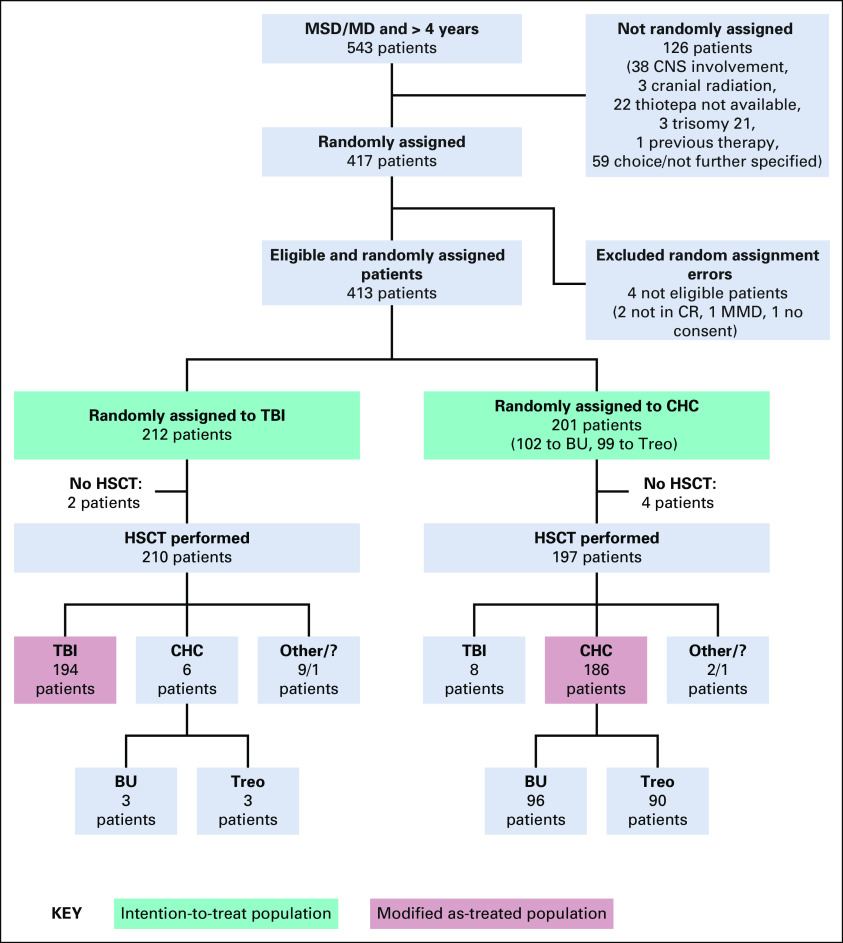
FORUM is a randomized, controlled, open-label, international, multicenter, phase III, noninferiority study. Patients ≤ 18 years at diagnosis, 4-21 years at HSCT, in complete remission pre-HSCT, and with an HLA-compatible related or unrelated donor were randomly assigned to myeloablative conditioning with fractionated 12 Gy TBI and etoposide versus fludarabine, thiotepa, and either busulfan or treosulfan. The noninferiority margin was 8%. With 1,000 patients randomly assigned in 5 years, 2-year minimum follow-up, and one-sided alpha of 5%, 80% power was calculated. A futility stopping rule would halt random assignment if chemoconditioning was significantly inferior to TBI (EudraCT: 2012-003032-22; ClinicalTrials.gov: NCT01949129).
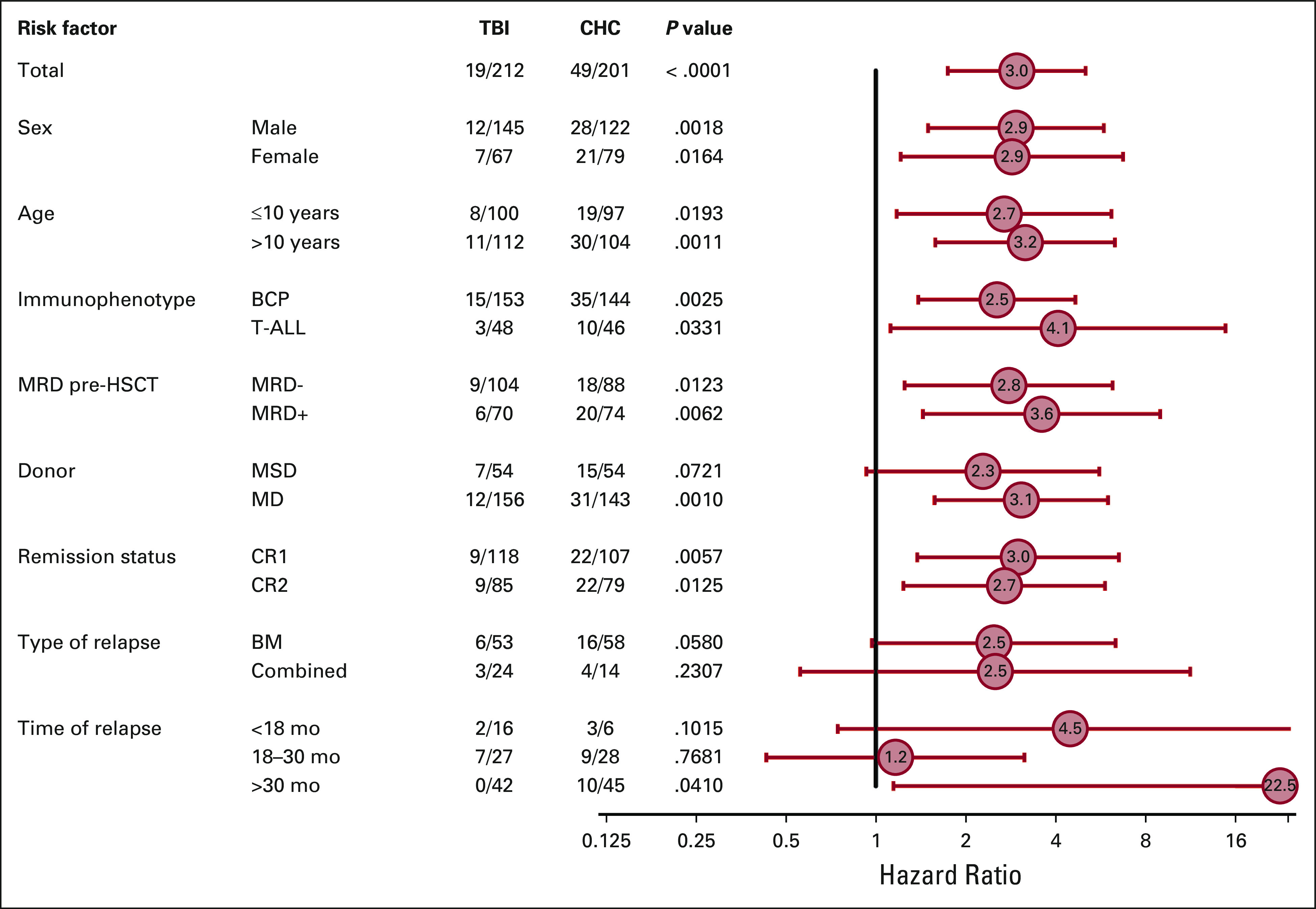
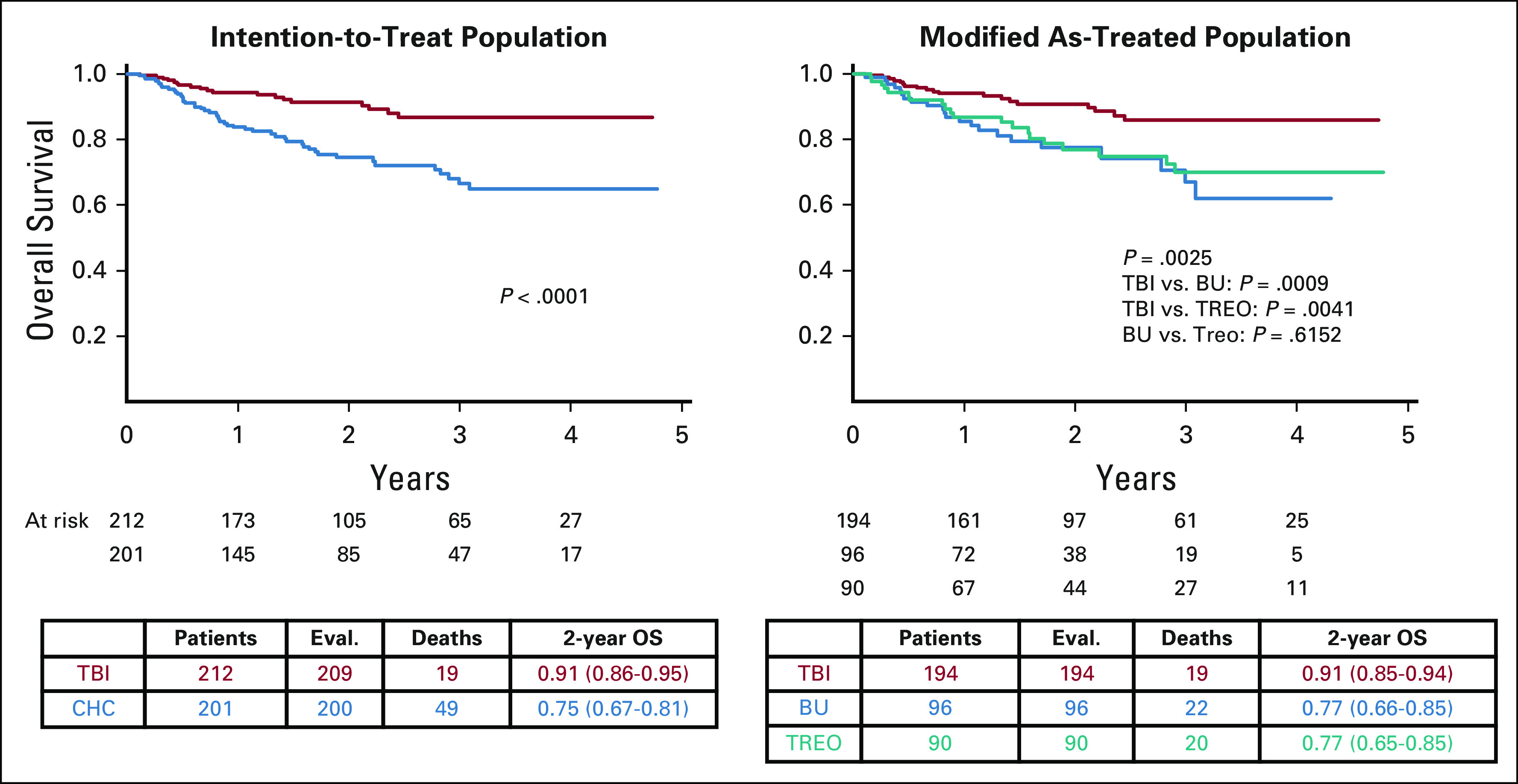
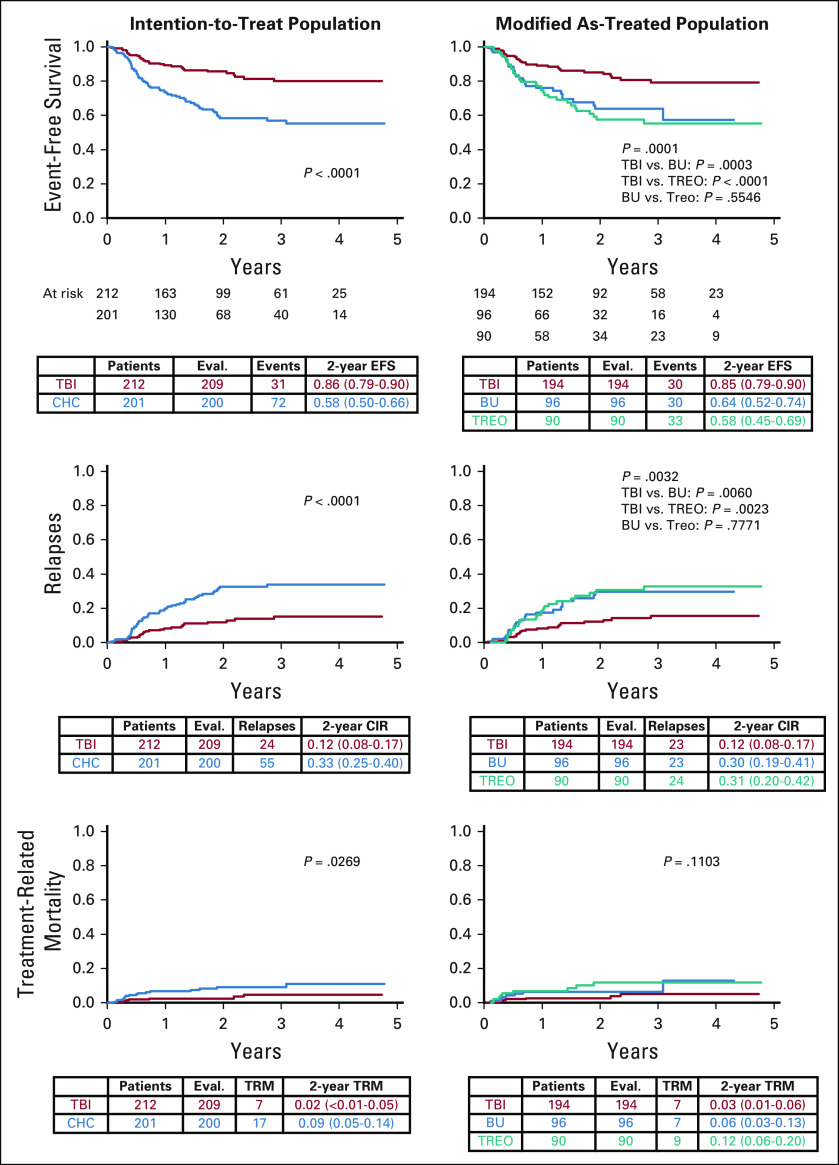
Between April 2013 and December 2018, 543 patients were screened, 417 were randomly assigned, 212 received TBI, and 201 received chemoconditioning. The stopping rule was applied on March 31, 2019. The median follow-up was 2.1 years. In the intention-to-treat population, 2-year overall survival (OS) was significantly higher following TBI (0.91; 95% CI, 0.86 to 0.95; < .0001) versus chemoconditioning (0.75; 95% CI, 0.67 to 0.81). Two-year cumulative incidence of relapse and treatment-related mortality were 0.12 (95% CI, 0.08 to 0.17; < .0001) and 0.02 (95% CI, < 0.01 to 0.05; = .0269) following TBI and 0.33 (95% CI, 0.25 to 0.40) and 0.09 (95% CI, 0.05 to 0.14) following chemoconditioning, respectively.
Improved OS and lower relapse risk were observed following TBI plus etoposide compared with chemoconditioning. We therefore recommend TBI plus etoposide for patients > 4 years old with high-risk ALL undergoing allogeneic HSCT.
全身放疗(TBI)在接受异基因造血干细胞移植(HSCT)的儿科急性淋巴细胞白血病(ALL)患者中是有效的,但长期的副作用令人担忧。我们研究了预处理联合化疗是否可以替代此类患者的 TBI。
FORUM 是一项随机、对照、开放标签、国际、多中心、III 期非劣效性研究。诊断时≤18 岁,HSCT 时 4-21 岁,HSCT 前完全缓解,且有 HLA 相容的相关或无关供者的患者被随机分配接受 12Gy 分次 TBI 和依托泊苷与氟达拉滨、噻替哌和布美他尼或替莫唑胺进行骨髓清除性预处理。非劣效性边界为 8%。在 5 年内随机分配 1000 例患者,最低随访 2 年,单侧 α 值为 5%,计算出 80%的效能。如果化学条件明显劣于 TBI(EudraCT:2012-003032-22;ClinicalTrials.gov:NCT01949129),则会停止随机分配。
2013 年 4 月至 2018 年 12 月,共筛选了 543 例患者,其中 417 例被随机分配,212 例接受了 TBI,201 例接受了化学预处理。2019 年 3 月 31 日应用了停止规则。中位随访时间为 2.1 年。在意向治疗人群中,TBI 组(0.91;95%CI,0.86 至 0.95;<.0001)的 2 年总生存率(OS)显著高于化疗组(0.75;95%CI,0.67 至 0.81)。TBI 组和化疗组的 2 年累积复发率和治疗相关死亡率分别为 0.12(95%CI,0.08 至 0.17;<.0001)和 0.02(95%CI,<0.01 至 0.05;=0.0269),0.33(95%CI,0.25 至 0.40)和 0.09(95%CI,0.05 至 0.14)。
与化疗相比,TBI 加依托泊苷可提高 OS 和降低复发风险。因此,我们建议对接受高危 ALL 异基因 HSCT 的>4 岁儿童患者使用 TBI 加依托泊苷。