Sampayo-Cordero Miguel, Miguel-Huguet Bernat, Pérez-García José, Páez David, Guerrero-Zotano Ángel L, Garde-Noguera Javier, Aguirre Elena, Holgado Esther, López-Miranda Elena, Huang Xin, Malfettone Andrea, Llombart-Cussac Antonio, Cortés Javier
Medica Scientia Innovation Research (MedSIR), Barcelona, Spain.
Medica Scientia Innovation Research (MedSIR), Ridgewood, NJ, USA.
Contemp Clin Trials Commun. 2020 Nov 28;20:100678. doi: 10.1016/j.conctc.2020.100678. eCollection 2020 Dec.
Non-inferiority (NI) analysis is not usually considered in the early phases of clinical development. In some negative phase II trials, a post-hoc NI analysis justified additional phase III trials that were successful. However, the risk of false positive achievements was not controlled in these early phase analyses. We propose to preplan NI analyses in superiority-based Simon's two-stage designs to control type I and II error rates.
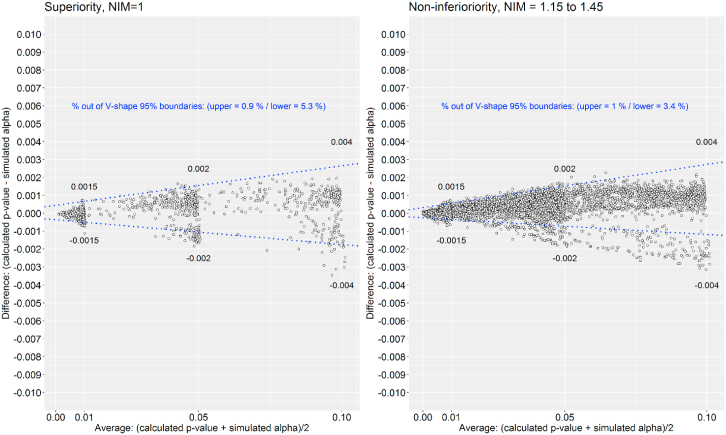
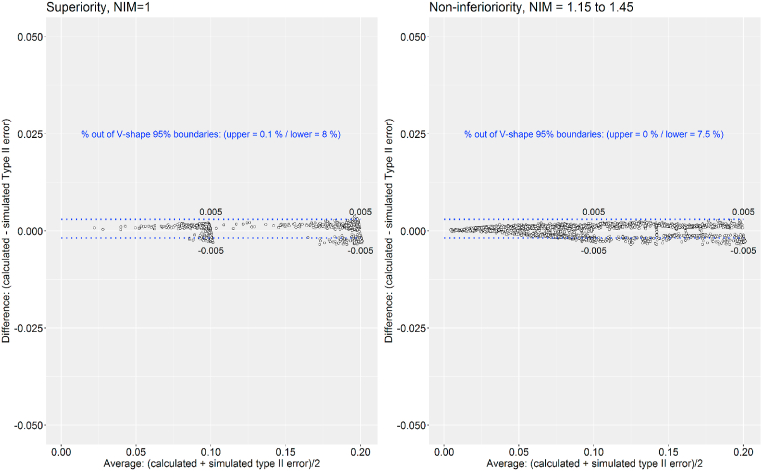
Simulations have been proposed to assess the control of type I and II errors rates with this method. A total of 12,768 two-stage Simon's design trials were constructed based on different assumptions of rejection response probability, desired response probability, type I and II errors, and NI margins. P-value and type II error were calculated with stochastic ordering using Uniformly Minimum Variance Unbiased Estimator. Type I and II errors were simulated using the Monte Carlo method. The agreement between calculated and simulated values was analyzed with Bland-Altman plots.
We observed the same level of agreement between calculated and simulated type I and II errors from both two-stage Simon's superiority designs and designs in which NI analysis was allowed. Different examples has been proposed to explain the utility of this method.
Inclusion of NI analysis in superiority-based single-arm clinical trials may be useful for weighing additional factors such as safety, pharmacokinetics, pharmacodynamic, and biomarker data while assessing early efficacy. Implementation of this strategy can be achieved through simple adaptations to existing designs for one-arm phase II clinical trials.
在临床开发的早期阶段,通常不会考虑非劣效性(NI)分析。在一些阴性的II期试验中,事后的NI分析为后续成功的III期试验提供了依据。然而,在这些早期分析中,假阳性结果的风险并未得到控制。我们建议在基于优效性的西蒙两阶段设计中预先规划NI分析,以控制I型和II型错误率。
已有人提出通过模拟来评估该方法对I型和II型错误率的控制情况。基于不同的拒绝反应概率、期望反应概率、I型和II型错误以及NI界值假设,构建了总共12768个两阶段西蒙设计试验。使用一致最小方差无偏估计器通过随机排序计算P值和II型错误。使用蒙特卡罗方法模拟I型和II型错误。通过布兰德-奥特曼图分析计算值与模拟值之间的一致性。
我们观察到,在两阶段西蒙优效性设计以及允许进行NI分析的设计中,计算得到的和模拟得到的I型和II型错误具有相同程度的一致性。已提出不同的示例来解释该方法的实用性。
在基于优效性的单臂临床试验中纳入NI分析,可能有助于在评估早期疗效时权衡其他因素,如安全性、药代动力学、药效学和生物标志物数据。通过对现有的单臂II期临床试验设计进行简单调整,即可实现该策略的实施。