Kathryn V. Papp, Center for Alzheimer Research and Treatment; 60 Fenwood Road; Boston, MA 02115, Telephone: 617-643-5322; Fax: 857-5461, Email Address:
J Prev Alzheimers Dis. 2021;8(1):59-67. doi: 10.14283/jpad.2020.38.
Computerized cognitive assessments may improve Alzheimer's disease (AD) secondary prevention trial efficiency and accuracy. However, they require validation against standard outcomes and relevant biomarkers.
To assess the feasibility and validity of the tablet-based Computerized Cognitive Composite (C3).
Cross-sectional analysis of cognitive screening data from the A4 study (Anti-Amyloid in Asymptomatic AD).
Multi-center international study.
Clinically normal (CN) older adults (65-85; n=4486).
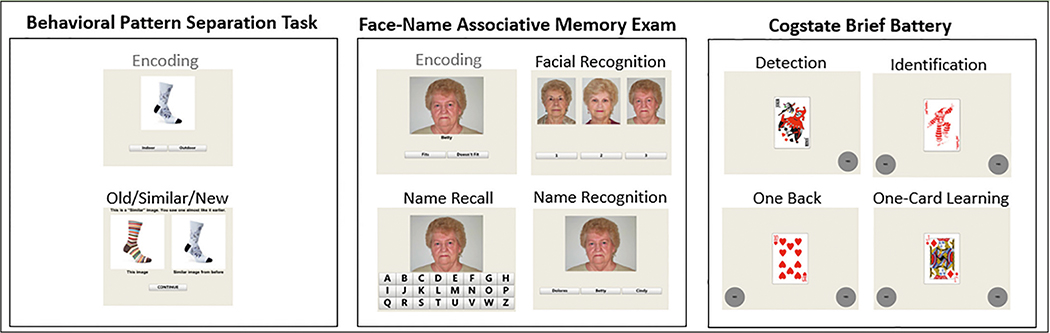
Participants underwent florbetapir-Positron Emission Tomography for Aβ+/- classification. They completed the C3 and standard paper and pencil measures included in the Preclinical Alzheimer's Cognitive Composite (PACC). The C3 combines memory measures sensitive to change over time (Cogstate Brief Battery-One Card Learning) and measures shown to be declining early in AD including pattern separation (Behavioral Pattern Separation Test- Object- Lure Discrimination Index) and associative memory (Face Name Associative Memory Exam- Face-Name Matching). C3 acceptability and completion rates were assessed using qualitative and quantitative methods. C3 performance was explored in relation to Aβ+/- groups (n=1323/3163) and PACC.
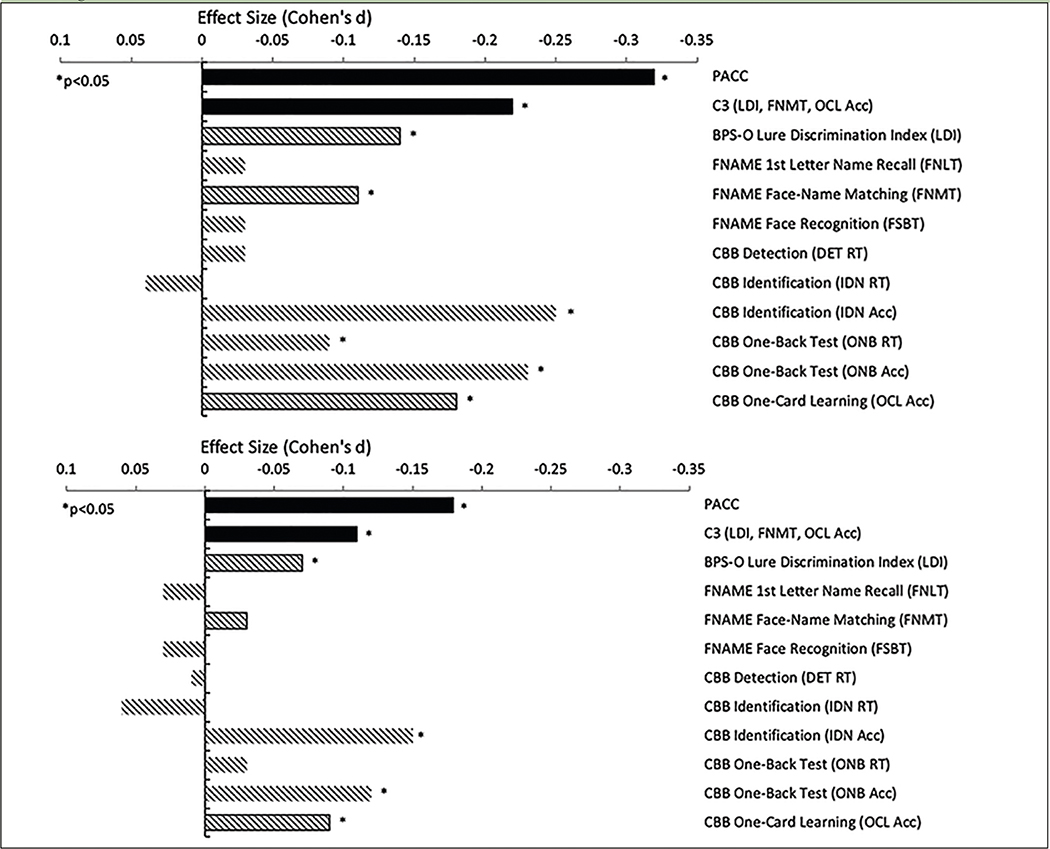
C3 was feasible for CN older adults to complete. Rates of incomplete or invalid administrations were extremely low, even in the bottom quartile of cognitive performers (PACC). C3 was moderately correlated with PACC (r=0.39). Aβ+ performed worse on C3 compared with Aβ- [unadjusted Cohen's d=-0.22 (95%CI: -0.31,-0.13) p<0.001] and at a magnitude comparable to the PACC [d=-0.32 (95%CI: -0.41,-0.23) p<0.001]. Better C3 performance was observed in younger, more educated, and female participants.
These findings provide support for both the feasibility and validity of C3 and computerized cognitive outcomes more generally in AD secondary prevention trials.
计算机认知评估可能会提高阿尔茨海默病(AD)二级预防试验的效率和准确性。然而,它们需要通过标准结果和相关生物标志物进行验证。
评估基于平板电脑的计算机认知综合测试(C3)的可行性和有效性。
A4 研究(无症状 AD 中的抗淀粉样蛋白)认知筛查数据的横断面分析。
多中心国际研究。
临床正常(CN)老年人(65-85 岁;n=4486)。
参与者接受氟比拉滨正电子发射断层扫描进行 Aβ+/ -分类。他们完成了 C3 以及标准纸笔测试,包括临床前阿尔茨海默病认知综合测试(PACC)。C3 结合了对随时间变化敏感的记忆测试(Cogstate 简短电池-一张卡片学习)和在 AD 早期表现出下降的测试,包括模式分离(行为模式分离测试-物体-诱饵辨别指数)和联想记忆(面孔名称联想记忆测试-面孔-名称匹配)。使用定性和定量方法评估 C3 的可接受性和完成率。探索 C3 与 Aβ+/ -组(n=1323/3163)和 PACC 的关系。
C3 对于 CN 老年人来说是可行的。即使在认知表现最差的四分之一(PACC),不完全或无效的管理率也非常低。C3 与 PACC 中度相关(r=0.39)。与 Aβ-相比,Aβ+在 C3 上的表现更差[未调整的 Cohen's d=-0.22(95%CI:-0.31,-0.13)p<0.001],与 PACC 相当[d=-0.32(95%CI:-0.41,-0.23)p<0.001]。在年龄较小、受教育程度较高和女性参与者中,C3 的表现更好。
这些发现为 C3 以及计算机认知结果在 AD 二级预防试验中的可行性和有效性提供了支持。