Roux Alexandre, Tran Stéphane, Edjlali Myriam, Saffroy Raphaël, Tauziede-Espariat Arnault, Zanello Marc, Gareton Albane, Dezamis Edouard, Dhermain Frédéric, Chretien Fabrice, Lechapt-Zalcman Emmanuèle, Oppenheim Catherine, Pallud Johan, Varlet Pascale
Service de Neurochirurgie, GHU Paris-Psychiatrie et Neurosciences-Hôpital Sainte-Anne, Paris, France.
Université de Paris, Sorbonne Paris Cité, Paris, France.
Brain Pathol. 2021 Jul;31(4):e12929. doi: 10.1111/bpa.12929. Epub 2021 Feb 15.
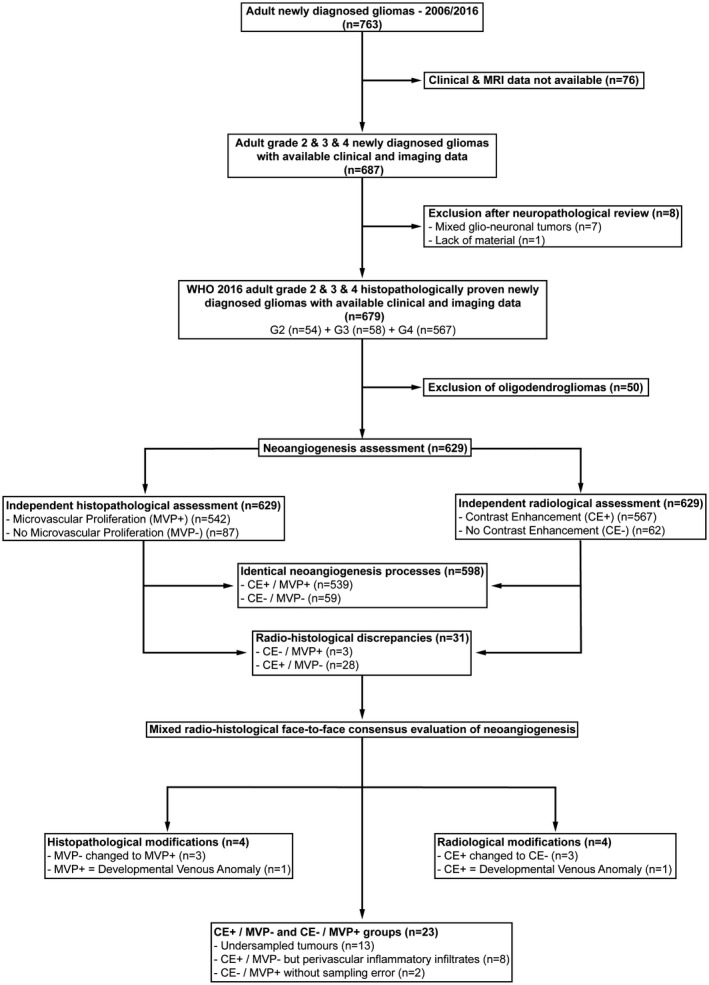
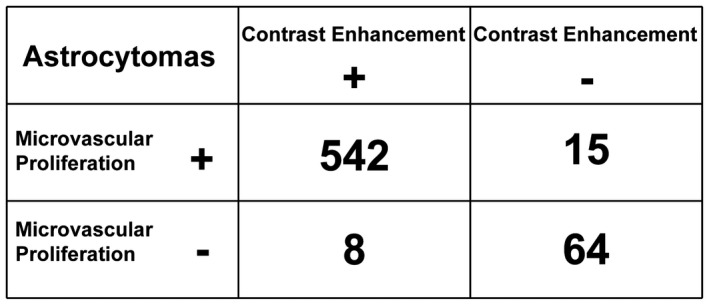
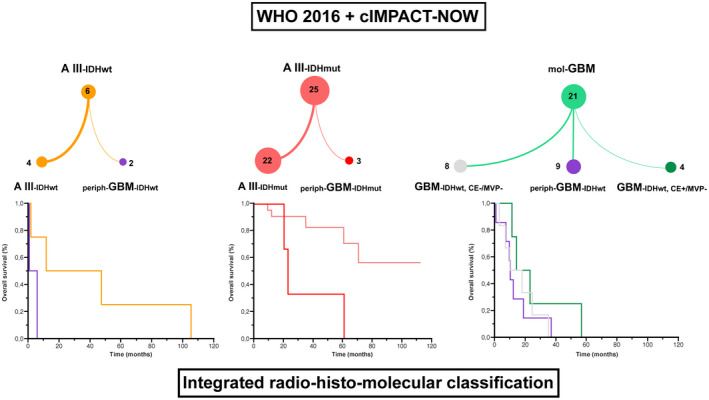
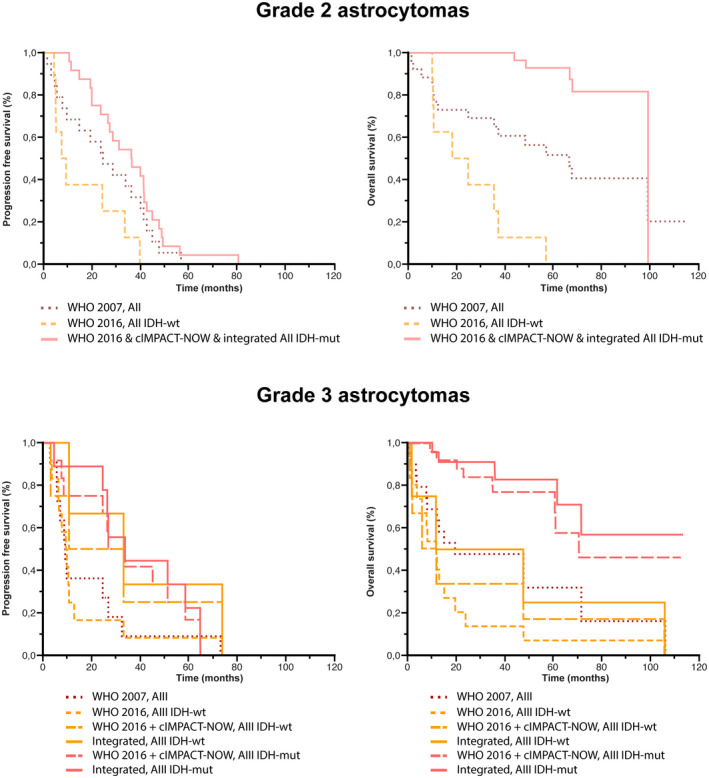
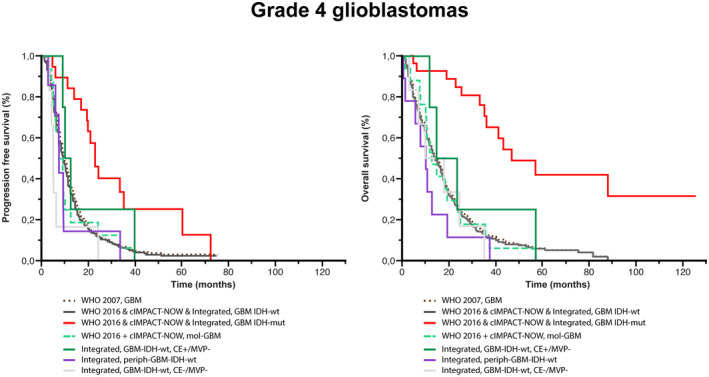
Assess the contribution of preoperative MRI data in improving grading of adult astrocytomas reclassified according to the WHO 2016 and cIMPACT-NOW update 3. Retrospective unicentric cohort study of 679 adult patients treated for newly diagnosed diffuse astrocytic and oligodendroglial tumors (January 2006-December 2016). We first systematically compared radiological (contrast enhancement present [CE+] vs. absent [CE-]) and histopathological findings (microvascular proliferation present [MPV+] vs. absent [MPV-]) to validate whether this comparing step of neoangiogenesis represents an efficient method to appreciate the representativity of the tumoral sampling. We focused on 629 cases of astrocytomas for radio-histological integrated analyses. In 598 cases (95.1%), neoangiogenesis evaluated by MRI or histology (CE+/MPV+ or CE-/MPV-) was identical. For the CE+/MPV- and CE-/MPV+ groups (23 cases), the radio-histological face-to-face evaluation allowed us to assess that for 13 cases (56.5%) the reason for this discrepancy was an undersampled tumor. We analyzed the group of CE+/MPV- (n = 8) and CE-/MPV+ (n = 2) in verified image-guided tumoral samples. Finally, we identified three new prognostic subgroups for molecular glioblastomas: (1) "non-representative sampling" (n = 9), (2) "Non neoangiogenic glioblastoma at the time of diagnosis, without contrast enhancement and microvascular proliferation" (n = 8), and (3) "contrast enhancing glioblastoma but without microvascular proliferation in a representative sample" (n = 4). Neoangiogenesis processes should be assessed to improve the prognosis accuracy of the current integrated diagnosis. We suggest adding imaging analyses during the neuropathological analysis of astrocytomas in adults.
评估术前MRI数据对改善根据世界卫生组织2016年分类及cIMPACT-NOW更新版3重新分类的成人星形细胞瘤分级的贡献。对679例新诊断的弥漫性星形细胞和少突胶质细胞瘤患者(2006年1月至2016年12月)进行回顾性单中心队列研究。我们首先系统地比较了放射学(有对比增强[CE+]与无对比增强[CE-])和组织病理学结果(有微血管增生[MPV+]与无微血管增生[MPV-]),以验证这种新血管生成的比较步骤是否是评估肿瘤取样代表性的有效方法。我们重点对629例星形细胞瘤病例进行放射-组织学综合分析。在598例病例(95.1%)中,通过MRI或组织学评估的新血管生成(CE+/MPV+或CE-/MPV-)是一致的。对于CE+/MPV-和CE-/MPV+组(23例),放射-组织学面对面评估使我们能够评估,在13例病例(56.5%)中,这种差异的原因是肿瘤取样不足。我们在经核实的影像引导肿瘤样本中分析了CE+/MPV-组(n = 8)和CE-/MPV+组(n = 2)。最后,我们确定了分子胶质母细胞瘤的三个新的预后亚组:(1)“非代表性取样”(n = 9),(2)“诊断时无新血管生成的胶质母细胞瘤,无对比增强和微血管增生”(n = 8),以及(3)“有对比增强的胶质母细胞瘤,但在代表性样本中无微血管增生”(n = 4)。应评估新血管生成过程以提高当前综合诊断的预后准确性。我们建议在成人星形细胞瘤的神经病理学分析过程中增加影像学分析。