Regenbogen Scott E, Cain-Nielsen Anne H, Syrjamaki John D, Norton Edward C
Department of Surgery, University of Michigan, Ann Arbor, Michigan.
Center for Healthcare Outcomes and Policy, University of Michigan, Ann Arbor, Michigan.
Ann Surg. 2021 Aug 1;274(2):199-205. doi: 10.1097/SLA.0000000000004726.
To evaluate real-world effects of enhanced recovery protocol (ERP) dissemination on clinical and economic outcomes after colectomy.
Hospitals aiming to accelerate discharge and reduce spending after surgery are increasingly adopting perioperative ERPs. Despite their efficacy in specialty institutions, most studies have lacked adequate control groups and diverse hospital settings and have considered only in-hospital costs. There remain concerns that accelerated discharge might incur unintended consequences.
Retrospective, population-based cohort including patients in 72 hospitals in the Michigan Surgical Quality Collaborative clinical registry (N = 13,611) and/or Michigan Value Collaborative claims registry (N = 14,800) who underwent elective colectomy, 2012 to 2018. Marginal effects of ERP on clinical outcomes and risk-adjusted, price-standardized 90-day episode payments were evaluated using mixed-effects models to account for secular trends and hospital performance unrelated to ERP.
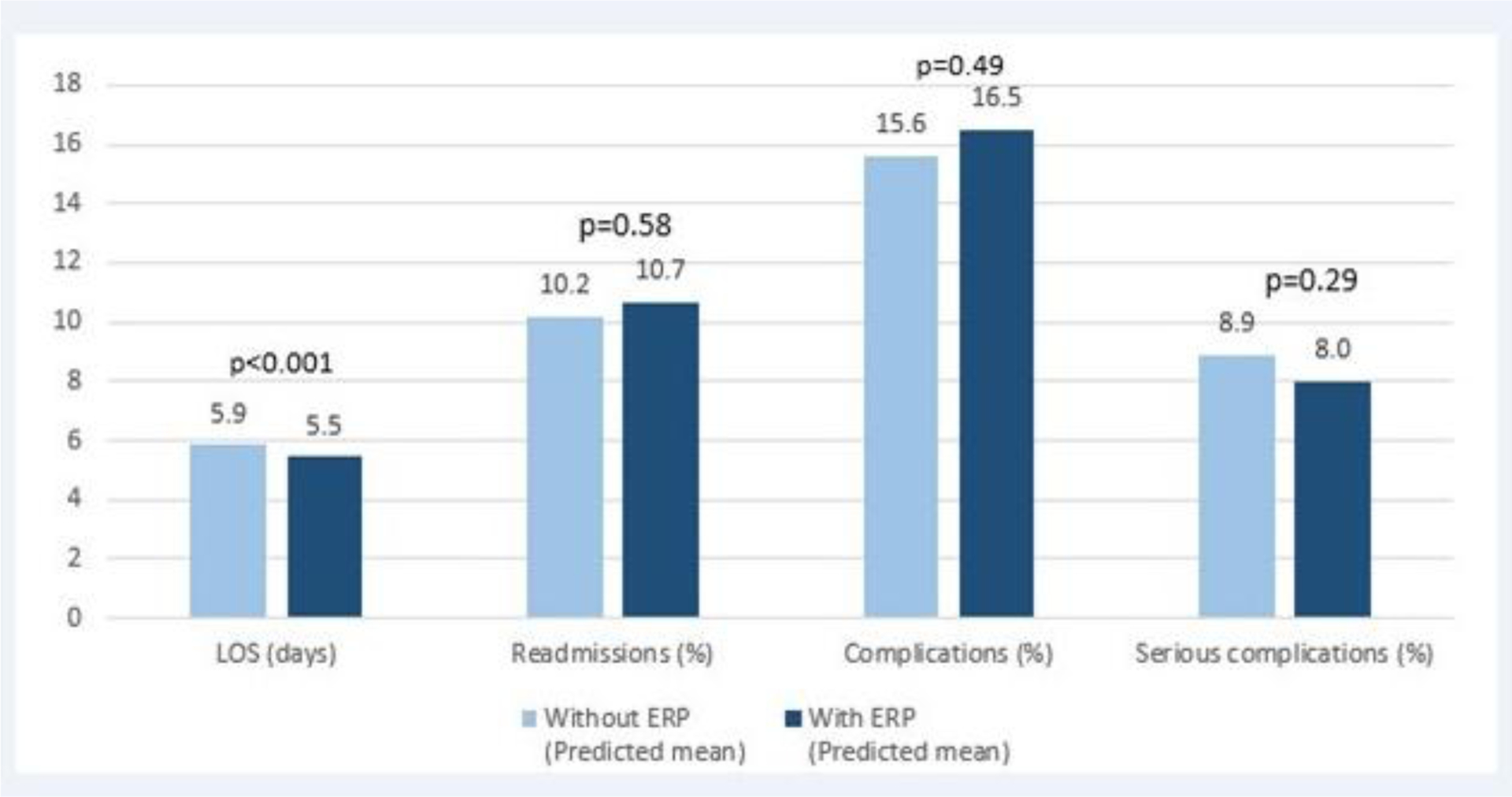
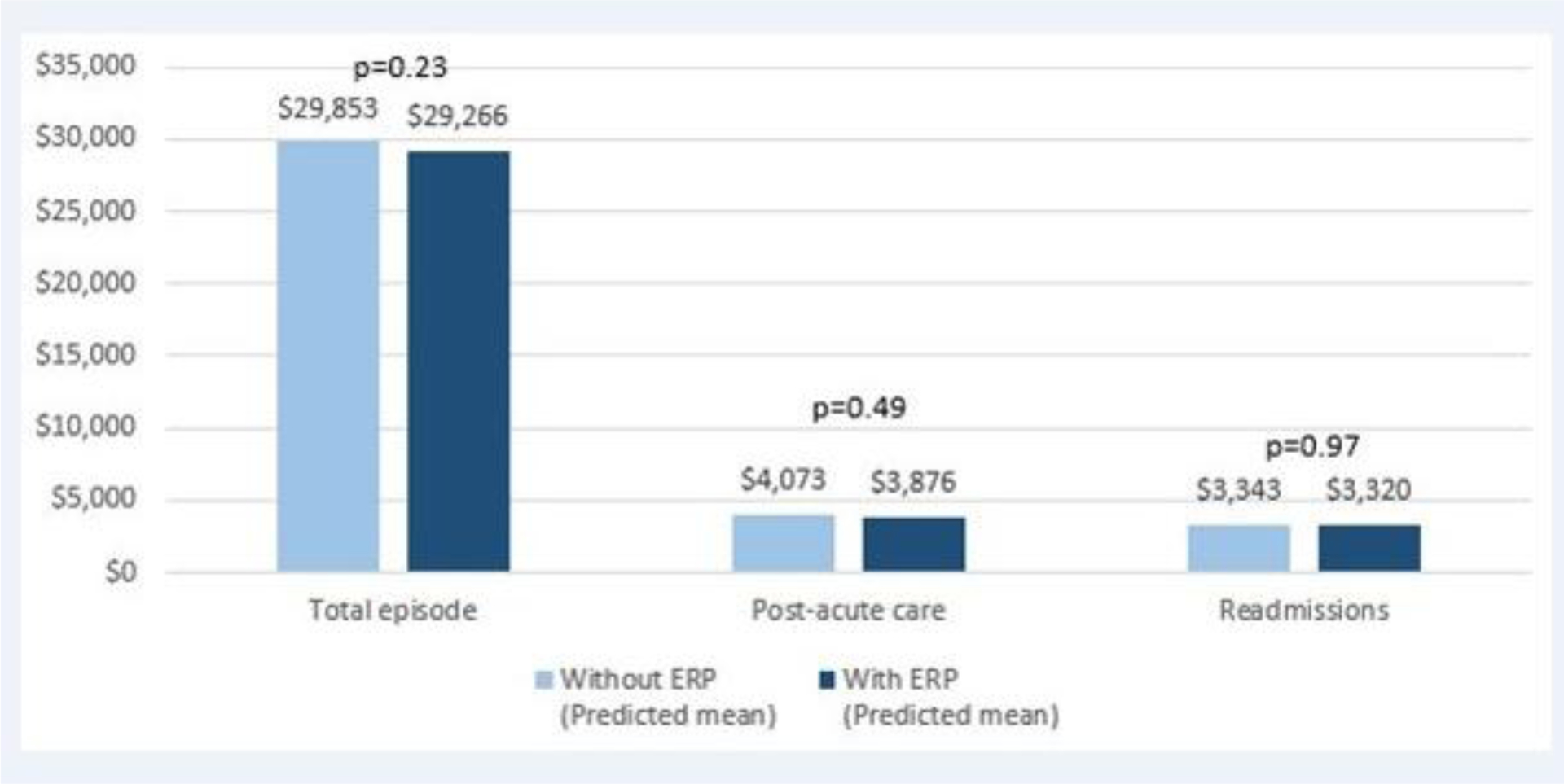
In 24 ERP hospitals, patients Post-ERP had significantly shorter length of stay than those Pre-ERP (5.1 vs 6.5 days, P < 0.001), lower incidence of complications (14.6% vs 16.9%, P < 0.001) and readmissions (10.4% vs 11.3%, P = 0.02), and lower episode payments ($28,550 vs $31,192, P < 0.001) and postacute care ($3,384 vs $3,909, P < 0.001). In mixed-effects adjusted analyses, these effects were significantly attenuated-ERP was associated with a marginal length of stay reduction of 0.4 days (95% confidence interval 0.2-0.6 days, P = 0.001), and no significant difference in complications, readmissions, or overall spending.
ERPs are associated with small reduction in postoperative length of hospitalization after colectomy, without unwanted increases in readmission or postacute care spending. The real-world effects across a variety of hospitals may be smaller than observed in early-adopting specialty centers.
评估强化康复方案(ERP)传播对结肠切除术后临床和经济结局的实际影响。
旨在加速出院并降低手术费用的医院越来越多地采用围手术期ERP。尽管其在专科医院有效,但大多数研究缺乏足够的对照组和多样化的医院环境,并且仅考虑了住院费用。人们仍然担心加速出院可能会产生意想不到的后果。
基于人群的回顾性队列研究,纳入2012年至2018年在密歇根外科质量协作临床登记处(N = 13,611)和/或密歇根价值协作索赔登记处(N = 14,800)的72家医院接受择期结肠切除术的患者。使用混合效应模型评估ERP对临床结局以及风险调整、价格标准化的90天发作期支付的边际效应,以考虑与ERP无关的长期趋势和医院绩效。
在24家采用ERP的医院中,ERP实施后患者的住院时间明显短于ERP实施前(5.1天对6.5天,P < 0.001),并发症发生率(14.6%对16.9%,P < 0.001)和再入院率(10.4%对11.3%,P = 0.02)更低,发作期支付(28,550美元对31,192美元,P < 0.001)和急性后期护理费用(3,384美元对3,909美元,P < 0.001)也更低。在混合效应调整分析中,这些效应明显减弱——ERP与住院时间边际缩短0.4天相关(95%置信区间0.2 - 0.6天,P = 0.001),并发症、再入院率或总体费用无显著差异。
ERP与结肠切除术后住院时间的小幅缩短相关,不会导致再入院率或急性后期护理费用意外增加。在各种医院中的实际效果可能比早期采用的专科医院观察到的要小。