Department of Critical Care Medicine, Tianjin Medical University General Hospital, Tianjin, China.
Advertising Center, Tianjin Daily, Tianjin, China.
BMJ Open. 2020 Dec 23;10(12):e041893. doi: 10.1136/bmjopen-2020-041893.
To develop and validate a prediction model for predicting in-hospital mortality in patients with acute pancreatitis (AP).
A retrospective observational cohort study based on a large multicentre critical care database.
All subject data were collected from the eICU Collaborative Research Database (eICU-CRD), which covers 200 859 intensive care unit admissions of 139 367 patients in 208 US hospitals between 2014 and 2015.
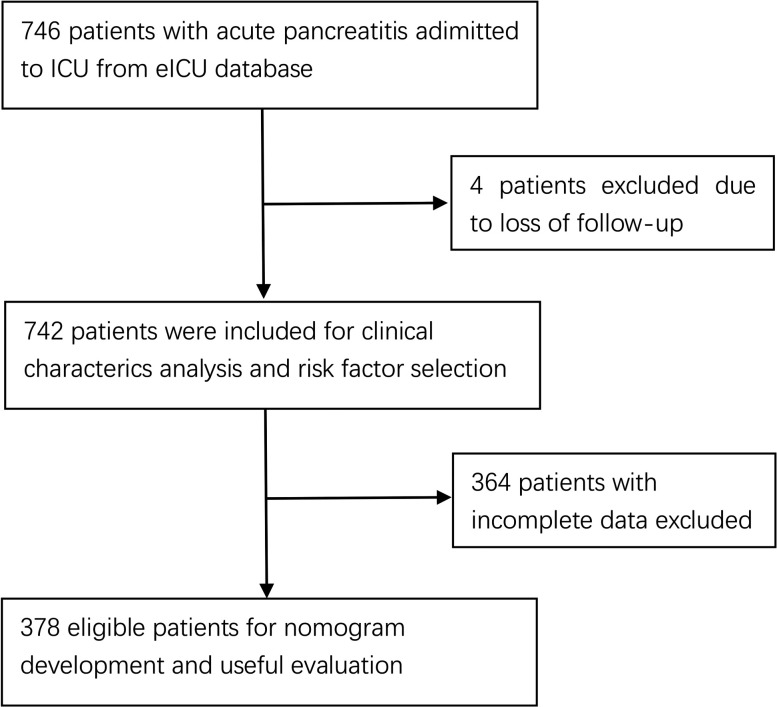
A total of 746 patients with AP were drawn from eICU-CRD. Due to loss to follow-up (four patients) or incomplete data (364 patients), 378 patients were enrolled in the primary cohort to establish a nomogram model and to conduct internal validation.
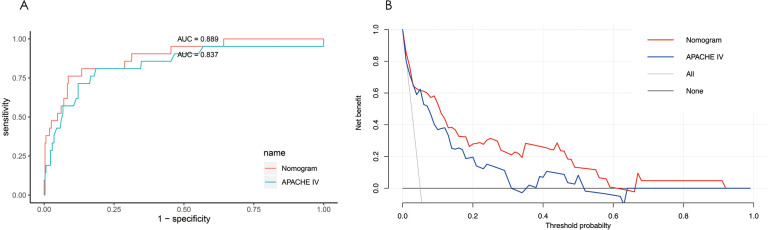
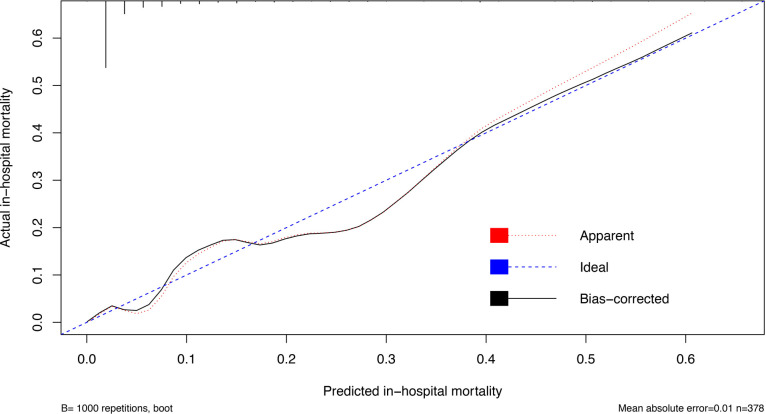
The outcome of the prediction model was in-hospital mortality. All risk factors found significant in the univariate analysis were considered for multivariate analysis to adjust for confounding factors. Then a nomogram model was established. The performance of the nomogram model was evaluated by the concordance index (C-index) and the calibration plot. The nomogram model was internally validated using the bootstrap resampling method. The predictive accuracy of the nomogram model was compared with that of Acute Physiology, Age, and Chronic Health Evaluation (APACHE) IV. Decision curve analysis (DCA) was performed to evaluate and compare the potential net benefit using of different predictive models.
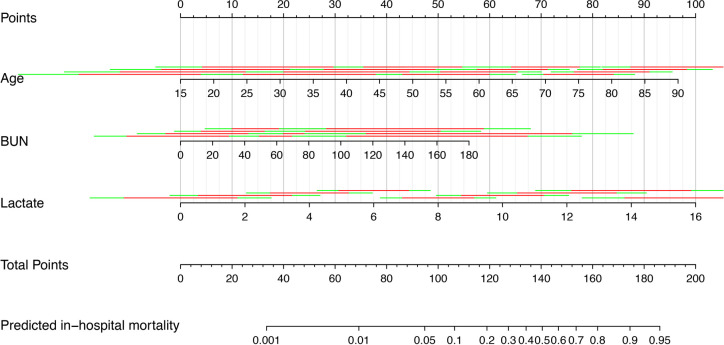
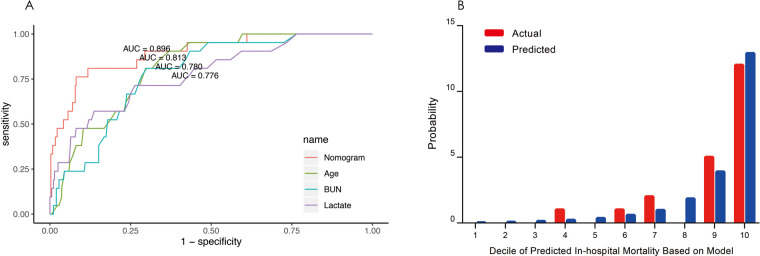
The overall in-hospital mortality rate is 4.447%. Age, BUN (blood urea nitrogen) and lactate (ABL) were the independent risk factors determined by multivariate analysis. The C-index of nomogram model ABL (0.896 (95% CI 0.825 to 0.967)) was similar to that of APACHE IV (p=0.086), showing a comparable discriminating power. Calibration plot demonstrated good agreement between the predicted and the actual in-hospital mortality. DCA showed that the nomogram model ABL was clinically useful.
Nomogram model ABL, which used readily available data, exhibited high predictive value for predicting in-hospital mortality in AP.
开发和验证用于预测急性胰腺炎(AP)患者住院死亡率的预测模型。
基于大型多中心重症监护数据库的回顾性观察队列研究。
所有研究数据均来自 eICU 协作研究数据库(eICU-CRD),该数据库涵盖了 2014 年至 2015 年间美国 208 家医院 139367 名患者的 200859 例重症监护室入住病例。
从 eICU-CRD 中抽取了 746 名患有 AP 的患者。由于随访丢失(4 名患者)或数据不完整(364 名患者),378 名患者被纳入主要队列以建立列线图模型并进行内部验证。
预测模型的结局是住院死亡率。在单因素分析中发现的所有有统计学意义的危险因素均被认为是多因素分析的混杂因素。然后建立了一个列线图模型。通过一致性指数(C 指数)和校准图评估列线图模型的性能。使用 bootstrap 重采样方法对内列线图模型进行验证。比较列线图模型与急性生理学、年龄和慢性健康评估(APACHE)IV 的预测准确性。决策曲线分析(DCA)用于评估和比较不同预测模型的潜在净获益。
总的住院死亡率为 4.447%。年龄、BUN(血尿素氮)和乳酸(ABL)是多因素分析确定的独立危险因素。列线图模型 ABL 的 C 指数为 0.896(95%CI 0.825 至 0.967),与 APACHE IV 相似(p=0.086),表明具有相当的区分能力。校准图显示预测和实际住院死亡率之间具有良好的一致性。DCA 显示列线图模型 ABL 具有临床实用性。
使用易于获得的数据的列线图模型 ABL 对预测 AP 患者住院死亡率具有较高的预测价值。