Cancer Biotherapy Unit, Department of Experimental Oncology, European Institute of Oncology IRCCS, Milan, Italy
Center for Immuno-Oncology, University Hospital of Siena; University of Siena, Siena, Italy.
J Immunother Cancer. 2020 Dec;8(2). doi: 10.1136/jitc-2020-001806.
In the KEYNOTE-022 study, pembrolizumab with dabrafenib and trametinib (triplet) improved progression-free survival (PFS) versus placebo with dabrafenib and trametinib (doublet) without reaching statistical significance. Mature results on PFS, duration of response (DOR), and overall survival (OS) are reported.
The double-blind, phase 2 part of KEYNOTE-022 enrolled patients with previously untreated -mutated advanced melanoma from 22 sites in seven countries. Patients were randomly assigned 1:1 to intravenous pembrolizumab (200 mg every 3 weeks) or placebo plus dabrafenib (150 mg orally two times per day) and trametinib (2 mg orally one time a day). Primary endpoint was PFS. Secondary endpoints were objective response rate, DOR, and OS. Efficacy was assessed in the intention-to-treat population, and safety was assessed in all patients who received at least one dose of study drug. This analysis was not specified in the protocol.
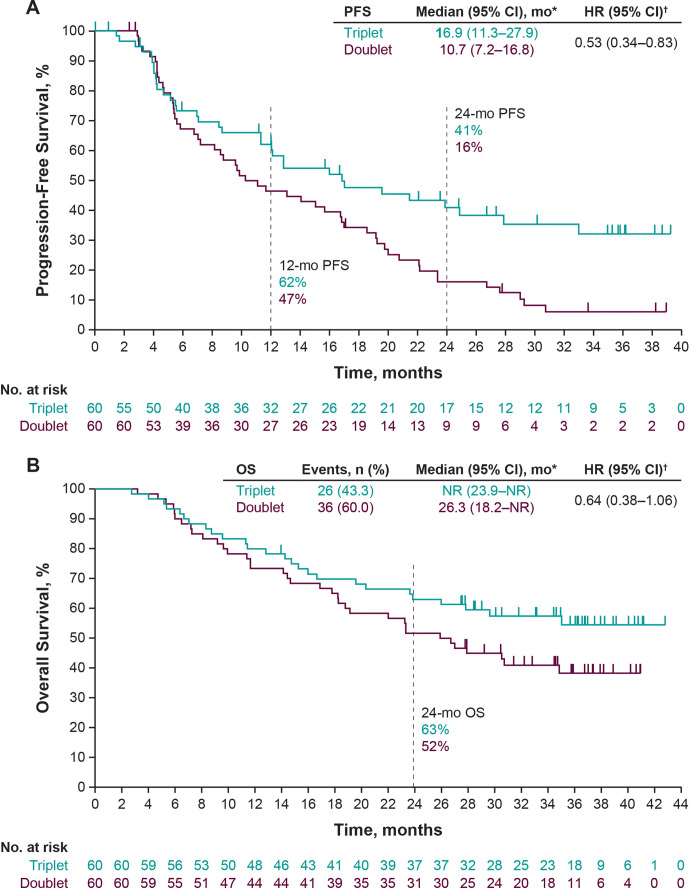
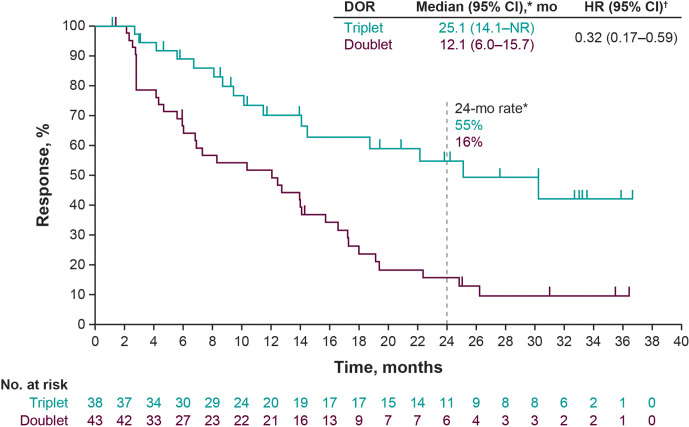
Between November 30, 2015 and April 24, 2017, 120 patients were randomly assigned to triplet (n=60) or doublet (n=60) therapy. With 36.6 months of follow-up, median PFS was 16.9 months (95% CI 11.3 to 27.9) with triplet and 10.7 months (95% CI 7.2 to 16.8) with doublet (HR 0.53; 95% CI 0.34 to 0.83). With triplet and doublet, respectively, PFS at 24 months was 41.0% (95% CI 27.4% to 54.2%) and 16.3% (95% CI 8.1% to 27.1%); median DOR was 25.1 months (95% CI 14.1 to not reached) and 12.1 months (95% CI 6.0 to 15.7), respectively. Median OS was not reached with triplet and was 26.3 months with doublet (HR 0.64; 95% CI 0.38 to 1.06). With triplet and doublet, respectively, OS at 24 months was 63.0% (95% CI 49.4% to 73.9%) and 51.7% (95% CI 38.4% to 63.4%). Grade 3-5 treatment-related adverse events (TRAEs) occurred in 35 patients (58%, including one death) receiving triplet and 15 patients (25%) receiving doublet.
In -mutant advanced melanoma, pembrolizumab plus dabrafenib and trametinib substantially improved PFS, DOR, and OS with a higher incidence of TRAEs. Interpretation of these results is limited by the post hoc nature of the analysis.
在 KEYNOTE-022 研究中,与安慰剂联合 dabrafenib 和 trametinib(双联组)相比,pembrolizumab 联合 dabrafenib 和 trametinib(三联组)改善了无进展生存期(PFS),但未达到统计学意义。现将 PFS、缓解持续时间(DOR)和总生存期(OS)的成熟结果报告如下。
KEYNOTE-022 的双盲、二期部分纳入了来自 7 个国家 22 个地点的未经治疗的-突变晚期黑色素瘤患者。患者按 1:1 随机分配接受静脉注射 pembrolizumab(每 3 周 200mg)或安慰剂联合 dabrafenib(每日两次,每次 150mg)和 trametinib(每日一次,每次 2mg)。主要终点为 PFS。次要终点包括客观缓解率、DOR 和 OS。在意向治疗人群中评估疗效,在接受至少一剂研究药物的所有患者中评估安全性。本分析未在方案中规定。
2015 年 11 月 30 日至 2017 年 4 月 24 日,120 名患者随机分配至三联组(n=60)或双联组(n=60)治疗。随访 36.6 个月,三联组中位 PFS 为 16.9 个月(95%CI 11.3 至 27.9),双联组为 10.7 个月(95%CI 7.2 至 16.8)(HR 0.53;95%CI 0.34 至 0.83)。分别接受三联组和双联组治疗的患者,24 个月时的 PFS 分别为 41.0%(95%CI 27.4%至 54.2%)和 16.3%(95%CI 8.1%至 27.1%);中位 DOR 分别为 25.1 个月(95%CI 14.1 至未达到)和 12.1 个月(95%CI 6.0 至 15.7)。三联组未达到中位 OS,双联组为 26.3 个月(HR 0.64;95%CI 0.38 至 1.06)。分别接受三联组和双联组治疗的患者,24 个月时的 OS 分别为 63.0%(95%CI 49.4%至 73.9%)和 51.7%(95%CI 38.4%至 63.4%)。三联组有 35 名患者(58%,包括 1 例死亡)和双联组 15 名患者(25%)发生 3-5 级治疗相关不良事件(TRAEs)。
在-突变的晚期黑色素瘤患者中,pembrolizumab 联合 dabrafenib 和 trametinib 显著改善了 PFS、DOR 和 OS,且 TRAEs 发生率较高。对这些结果的解释受到分析的事后性质的限制。