Qiu Jianhui, Zhang Kenan, Ma Kaifang, Zhou Jingcheng, Gong Yanqing, Cai Lin, Gong Kan
Department of Urology, Peking University First Hospital, Beijing, China.
Institute of Urology, Peking University, Beijing, China.
Front Genet. 2020 Dec 10;11:532588. doi: 10.3389/fgene.2020.532588. eCollection 2020.
Von Hippel-Lindau (VHL) disease is a hereditary kidney cancer syndrome, with which patients are more likely to get affected by renal cell carcinoma (RCC), pancreatic cyst or tumor (PCT), central nervous system hemangioblastoma (CHB), retinal angiomas (RA), and pheochromocytoma (PHEO). Mutations of VHL gene located in 3p25 may impair the function of the VHL protein and lead to the disease. It's unclear why obvious phenotype varieties exist among VHL patients. Here we aimed to ascertain whether the mutation types and locations affect the phenotype.
We enrolled 577 Chinese VHL patients from 211 families and divided them into three groups and six subgroups according to their mutation types and locations. Cox survival analysis and Kaplan-Meier analysis were used to compare intergroup age-related tumor risks.
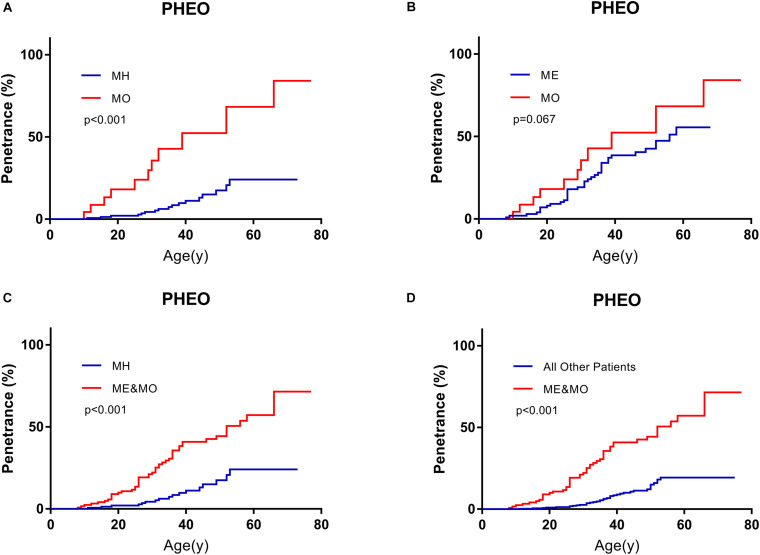
Patients with nonsense or frameshift mutations that were located before residues 117 of VHL protein (NoF1 subgroup) hold lower age-related risks of VHL associated tumors ( = 0.638, 95%CI 0.461-0.883, = 0.007), CHB ( = 0.596, 95%CI 0.409-0.868, = 0.007) or PCT ( = 0.595, 95%CI 0.368-0.961, = 0.034) than patients whose mutations were located after residues 117 (NoF2 subgroup). Patients in NoF1 subgroup still had lower age-related risks of CHB ( = 0.652, 95%CI 0.476-0.893, = 0.008) and PCT ( = 0.605, 95%CI 0.398-0.918, = 0.018) compared with those in combined NoF2 subgroup and other truncating mutation patients. NoF1 subgroup correspondingly had a longer estimated median lifespan (64 vs. 55 year, = 0.037) than NoF2 subgroup. Among patients with missense mutations of VHL, only a small minority (23 of 286 missense mutations carriers) carried mutations involving neither HIF-α binding region nor elongin C binding region, who were grouped in MO subgroup. MO subgroup seemed to have a higher age-related risk of PHEO. In the whole cohort ( = 577), PHEO was an independent protective factor for CHB ( = 0.001) and survival ( = 0.005). RA and CHB failed to predict the age-related risk of each other.
The mutation types and locations of VHL gene are associated with phenotypes. Genetic counselors could predict phenotypes more accurately based on more detailed genotype-phenotype correlations. Further genotype-phenotype studies should focus on the prediction of tumor recurrence, progression, and metastasis. The deep molecular mechanism of genotype-phenotype correlation is worth further exploring.
冯·希佩尔-林道(VHL)病是一种遗传性肾癌综合征,患者更易患肾细胞癌(RCC)、胰腺囊肿或肿瘤(PCT)、中枢神经系统血管母细胞瘤(CHB)、视网膜血管瘤(RA)和嗜铬细胞瘤(PHEO)。位于3p25的VHL基因突变可能损害VHL蛋白功能并导致该病。目前尚不清楚为何VHL患者之间存在明显的表型差异。本研究旨在确定突变类型和位置是否影响表型。
我们招募了来自211个家庭的577例中国VHL患者,并根据其突变类型和位置将他们分为三组和六个亚组。采用Cox生存分析和Kaplan-Meier分析比较组间与年龄相关的肿瘤风险。
VHL蛋白第117位残基之前发生无义或移码突变的患者(NoF1亚组)与VHL相关肿瘤(=0.638,95%CI 0.461-0.883,=0.007)、CHB(=0.596,95%CI 0.409-0.868,=0.007)或PCT(=0.595,95%CI 0.368-0.961,=0.034)的年龄相关风险低于突变位于第117位残基之后的患者(NoF2亚组)。与NoF2亚组合并其他截短突变患者相比,NoF1亚组患者的CHB(=0.652,95%CI 0.476-0.893,=0.008)和PCT(=0.605,95%CI 0.398-0.918,=0.018)年龄相关风险仍较低。NoF1亚组的估计中位寿命相应比NoF2亚组长(64岁对55岁,=0.037)。在VHL错义突变患者中,只有一小部分(286名错义突变携带者中的23名)携带的突变既不涉及HIF-α结合区域也不涉及延伸蛋白C结合区域,这些患者被归入MO亚组。MO亚组似乎患PHEO的年龄相关风险更高。在整个队列(=577)中,PHEO是CHB(=0.001)和生存(=0.005)的独立保护因素。RA和CHB未能相互预测年龄相关风险。
VHL基因的突变类型和位置与表型相关。遗传咨询师可根据更详细的基因型-表型相关性更准确地预测表型。进一步的基因型-表型研究应侧重于肿瘤复发、进展和转移的预测。基因型-表型相关性的深层分子机制值得进一步探索。