Department of Medical Sciences, Uppsala University, Uppsala, Sweden.
Uppsala Clinical Research Center, Uppsala, Sweden.
Eur Heart J. 2021 Jan 20;42(3):243-252. doi: 10.1093/eurheartj/ehaa1011.
Clinical trials have demonstrated that a reduction in low-density lipoprotein cholesterol (LDL-C) reduces cardiovascular (CV) events. This has, however, not yet been shown in a real-world setting. We aimed to investigate the association between LDL-C changes and statin intensity with prognosis after a myocardial infarction (MI).
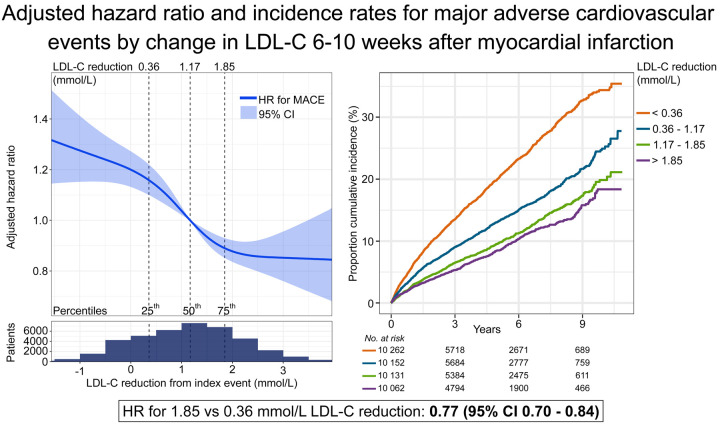
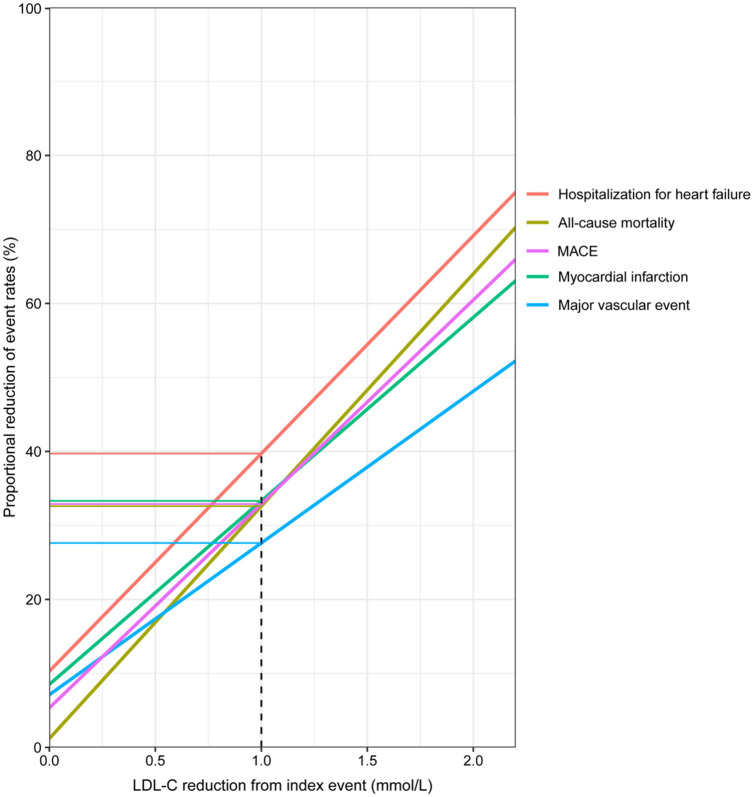
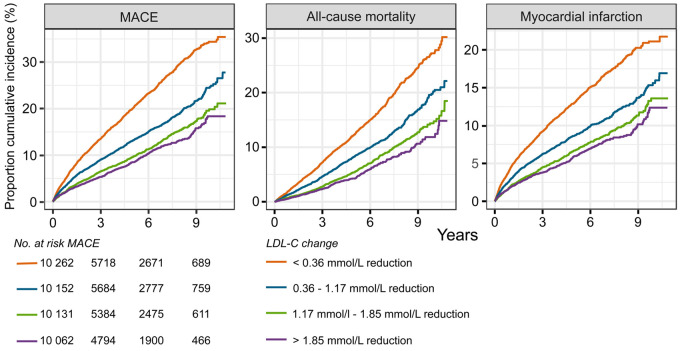
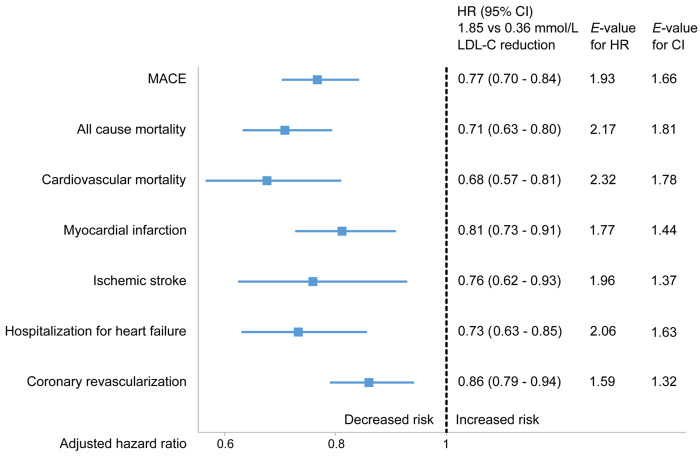
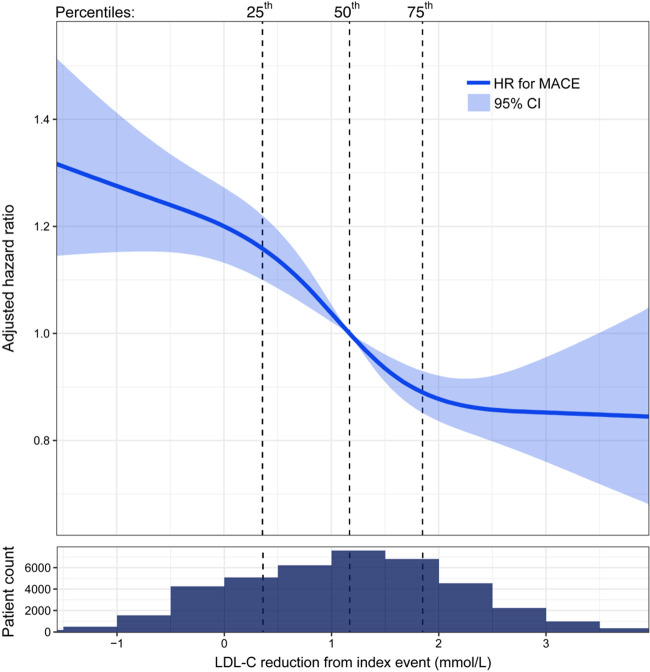
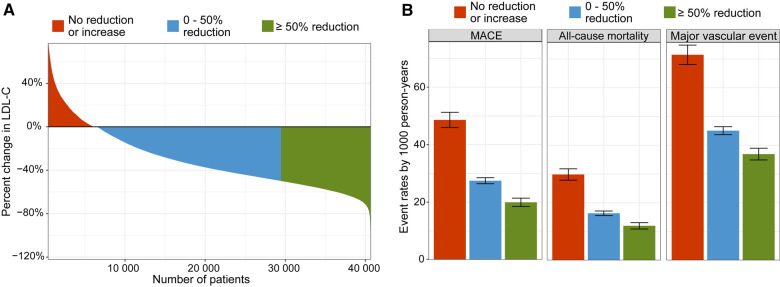
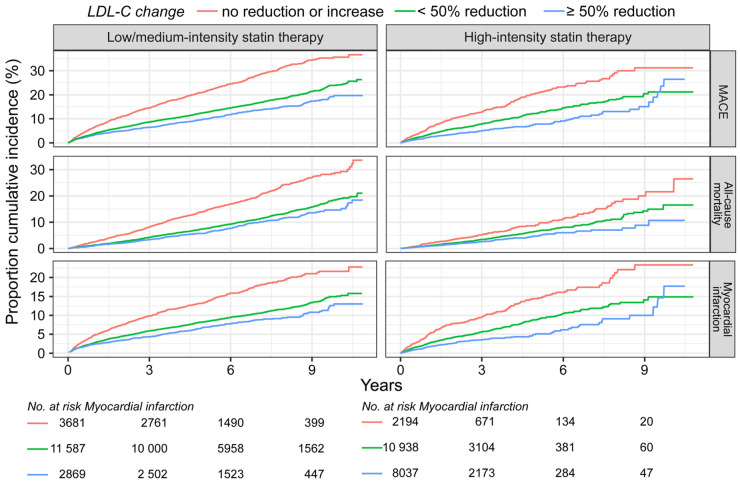
Patients admitted with MI were followed for mortality and major CV events. Changes in LDL-C between the MI and a 6- to 10-week follow-up visit were analysed. The associations between quartiles of LDL-C change and statin intensity with outcomes were assessed using adjusted Cox regression analyses. A total of 40 607 patients were followed for a median of 3.78 years. The median change in LDL-C was a 1.20 mmol/L reduction. Patients with larger LDL-C reduction (1.85 mmol/L, 75th percentile) compared with a smaller reduction (0.36 mmol/L, 25th percentile) had lower hazard ratios (HR) for all outcomes (95% confidence interval): composite of CV mortality, MI, and ischaemic stroke 0.77 (0.70-0.84); all-cause mortality 0.71 (0.63-0.80); CV mortality 0.68 (0.57-0.81); MI 0.81 (0.73-0.91); ischaemic stroke 0.76 (0.62-0.93); heart failure hospitalization 0.73 (0.63-0.85), and coronary artery revascularization 0.86 (0.79-0.94). Patients with ≥50% LDL-C reduction using high-intensity statins at discharge had a lower incidence of all outcomes compared with those using a lower intensity statin.
Larger early LDL-C reduction and more intensive statin therapy after MI were associated with a reduced hazard of all CV outcomes and all-cause mortality. This supports clinical trial data suggesting that earlier lowering of LDL-C after an MI confers the greatest benefit.
临床试验已经证明,降低低密度脂蛋白胆固醇(LDL-C)可减少心血管(CV)事件。然而,这尚未在真实环境中得到证实。我们旨在研究 LDL-C 变化与他汀类药物强度与心肌梗死(MI)后预后之间的关系。
对 MI 入院患者进行死亡率和主要 CV 事件随访。分析 MI 和 6 至 10 周随访期间 LDL-C 的变化。使用调整后的 Cox 回归分析评估 LDL-C 变化和他汀类药物强度的四分位与结局之间的关系。共随访了 40607 例患者,中位随访时间为 3.78 年。LDL-C 的中位数变化为降低 1.20mmol/L。与较小的 LDL-C 降低(0.36mmol/L,25 百分位)相比,较大的 LDL-C 降低(1.85mmol/L,75 百分位)的患者所有结局的危险比(HR)均较低(95%置信区间):心血管死亡率、MI 和缺血性卒中的复合结局为 0.77(0.70-0.84);全因死亡率为 0.71(0.63-0.80);心血管死亡率为 0.68(0.57-0.81);MI 为 0.81(0.73-0.91);缺血性卒变为 0.76(0.62-0.93);心力衰竭住院率为 0.73(0.63-0.85),冠状动脉血运重建率为 0.86(0.79-0.94)。出院时使用高强度他汀类药物达到≥50%LDL-C 降低的患者与使用低强度他汀类药物的患者相比,所有结局的发生率均较低。
MI 后更大的早期 LDL-C 降低和更强化的他汀类药物治疗与所有 CV 结局和全因死亡率的降低相关。这支持临床试验数据表明,MI 后更早降低 LDL-C 可带来最大获益。